Clinical Summary
A 72-year-old woman with no significant history presents with a 4.0 cm eczematous, slowly spreading plaque in the vulvar area.
Master List
- Extramammary Paget disease
- Melanoma in situ
- Merkel cell carcinoma in situ
- Pagetoid Bowen disease
- Sebaceous carcinoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2013, case 21, and is extramammary Paget disease.
Criteria for Diagnosis and Comments
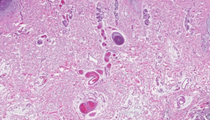
Sections show a broad intraepidermal proliferation composed of atypical cells with abundant pale cytoplasm and large vesicular nuclei. Some atypical cells appear to contain bluish granular material within the cytoplasm suggestive of mucin. Occasional atypical cells with intracellular brown pigment consistent with melanin are also noted. The cells are distributed as single units or clusters scattered at various levels throughout the epidermis. Atypical cells are also seen involving the contiguous epithelium of hair follicles and sweat ducts. Within the superficial dermis there is fibrosis and chronic inflammation and in some areas there are small clusters and single cells with similar morphology to the intraepidermal Paget cells. Based on the histological features the correct diagnosis among the presented choices is extramammary Paget disease.
Paget disease of the nipple and areola was initially reported in 1874 by Sir James Paget who described eczema-like lesions involving the breast of 15 women who subsequently developed breast carcinoma. Paget disease is encountered in approximately 1–5% of all mammary carcinomas and rarely may represent the initial sign of an underlying breast adenocarcinoma. It usually occurs from intraepidermal extension of intraductal breast carcinoma without destruction of the epidermal basement membrane. The first case of extramammary Paget disease (EMPD) involving the male genitalia was reported by Crocker et al in 1889. EMPD is a rare entity, less common than the mammary counterpart, presenting in areas rich in apocrine glands such as vulva and perianal region. Less often, EMPD has been reported involving the penis, scrotum, axilla, eyelid and external auditory canal. Rarely, multifocal cases involving both axillae and genital area, called triple EMPD, are known to occur. EMPD presents with single or multiple erythematous, well-demarcated, pruritic or painful plaques with erosions or ulcerations. The lesions may have an eczematous appearance which could delay the diagnosis. In later stages tumor nodules may develop. There are reports of EMPD presenting with pigmented plaques (pigmented EMPD) mimicking a melanocytic lesion.
In the majority of cases, EMPD presents as a primary epidermal neoplasm without an associated invasive carcinoma. In a minority of cases (about 25%), EMPD represents an epidermotropic extension from an underlying adnexal sweat gland carcinoma, most commonly of apocrine differentiation, although rarely eccrine lesions have been described. EMPD involving the external auditory canal occurs in association with a ceruminous carcinoma while EMPD on the eyelids is associated with carcinoma of Moll's glands. Less often, EMPD may also be a manifestation of a cutaneous metastasis from a more distant neoplasm such as carcinoma of the prostate, rectum, urethra, bladder, cervix, or stomach.
While the pathogenesis of secondary EMPD is related to the intraepidermal spread of the underlying carcinoma, the pathogenesis of EMPD not associated with an underlying carcinoma (primary EMPD) is less clear. It is believed to represent an in situ malignancy derived from the intraepidermal portion of the sweat duct. Other theories suggest that EMPD may arise from pluripotential cells located in the epidermis or from the Toker cells which have been identified in the vulval epidermis. Another hypothesis states that EMPD could result from the adnexal stem cells located in the infundibulo-sebaceous unit of the hair follicle, since Paget cells express cytokeratins 15 and 19 which are markers of follicular stem cells from the hair bulge region.
Histologic examination of EMPD shows infiltration of the epidermis by large cells with abundant clear or eosinophilic cytoplasm, distributed singly or in clusters at various levels of the epidermis. The atypical cells are concentrated in the lower half of the epidermis; however, in some areas the entire thickness of the epidermis may be involved. The cells have large pleomorhic nuclei and prominent nucleoli. Occasionally glandular differentiation or signet ring cells may be seen. In the pigmented variant of EMPD a large number of tumor cells contain melanin pigment and there is also an increase in epidermal dendritic melanocytes (current case focally demonstrates this feature). In the anogenital region, EMPD may be associated with epidermal hyperplasia in the form of papillomatosis or lesions mimicking fibroepithelioma of Pinkus, which when present may hide the histological features of EMPD. Rarely, EMPD may evolve to invasive disease, characterized by Paget cells within the dermis. Secondary EMPD is associated with an underlying in-situ or invasive adnexal carcinoma, usually with apocrine differentiation, or with a more distant carcinoma.
The tumor cells usually contain mucin and are PAS diastase-resistant, mucicarmine and alcian blue at pH 2.5 positive. By immunohistochemistry, EMPD cells express low molecular weight cytokeratins (CK7, Cam 5.2), AE1/AE3, and EMA. About 50% of EMPD cases are positive for GCDFP-15 (usually positive in primary disease) and there is variable expression of CEA. Primary EMPD is positive for MUC1 and MUC5AC and negative for MUC2, while secondary EMPD is less likely to express MUC5AC and may label with MUC2 (cases associated with rectal adenocarcinoma). EMPD is also reported to express androgen receptor and HER-2/neu in some cases, raising the possibility for targeted therapy, however they are usually negative for estrogen and progesterone receptors by immunohistochemistry. Recently, CD23 has been found to be expressed in EMPD (and also in mammary Paget disease) and was negative in lesions in the differential diagnosis including Bowen disease, melanoma in situ, and sebaceous carcinoma, thus is being proposed as a useful diagnostic marker. Similarly, RCAS1 (receptor-binding cancer antigen expressed by SiSo cells) has been reported as a sensitive marker for EMPD, however it is also expressed in squamous cell carcinoma.
Treatment of choice for EMPD is surgical excision with large margins or even vulvectomy or abdomino-perineal resection. Even with treatment, local recurrences are quite common ranging from 33% to 60%, mainly due to the extension of the lesion beyond the clinically abnormal area. The prognosis is relatively good in the primary cases however mortality is as high as 50% in EMPD associated with an underlying adnexal or visceral carcinoma. Poor prognosis is also associated with nodules in the primary lesion, elevated serum CEA levels, tumor invasion level and presence of lymph node metastases.
Differential diagnosis of EMPD includes other tumors characterized by a prominent pagetoid intraepidermal pattern including melanoma in situ, pagetoid squamous cell carcinoma in situ (pagetoid Bowen disease), sebaceous carcinoma, and Merkel cell carcinoma. Melanoma in situ may mimic clinically and histologically EMPD, especially the pigmented variant. However, by immunohistochemistry, melanoma is easily differentiated from EMPD based on the negative expression of melanocytic markers HMB-45, S100, and Mart-1 in EMPD. Pagetoid squamous cell carcinoma in situ (pagetoid Bowen disease) is characterized by nests of cells with pale cytoplasm within areas of normal epidermis, resembling EMPD by histology. However, in pagetoid Bowen disease, the lesional cells demonstrate higher grade atypia than those of EMPD and intercellular bridges are seen. Also Bowen disease is usually negative for Cam5.2, GCDFP-15, Her-2/neu, BerEP4, and mucin stains and positive for p63, while the reverse is true for EMPD. CK7 labels most EMPD cases; however, recently, Bowen disease has also been reported to be positive for CK7 in some cases. Sebaceous carcinoma is another tumor that can exhibit a pagetoid intraepidermal pattern (in about one third of cases in one study). While an invasive dermal sebaceous carcinoma component is usually also present, in superficial biopsies the invasive component may be unapparent and the lesion may mimic EMPD. By histology, sebaceous carcinomas contain cytoplasmic vacuoles. Adipophilin has been recently reported to be expressed in a membranous vesicular pattern in sebaceous tumors including sebaceous carcinoma and may serve as a marker for this entity. Merkel cell carcinoma is known to exhibit intraepidermal pagetoid spread and rarely purely intraepidermal (in situ) tumors have been described. As opposed to EMPD, Merkel cell carcinoma demonstrates a neuroendocrine histology with large nuclei with "salt and pepper" chromatin, little cytoplasm, and numerous mitotic figures.
Supplementary Questions
- Which one of the following statements regarding the most common presentation of extramammary Paget disease (EMPD) is true?
- EMPD is usually a manifestation of a cutaneous metastasis from prostate carcinoma
- EMPD is usually a manifestation of a cutaneous metastasis from rectal carcinoma
- EMPD usually presents as a primary epidermal neoplasm without an associated carcinoma
- EMPD usually represents an epidermotropic extension from an underlying apocrine carcinoma
- EMPD is usually a manifestation of a cutaneous metastasis from gastric carcinoma
- Which one of the following markers is usually expressed in EMPD?
- Androgen receptor
- EGFR
- Estrogen receptor
- p63
- Progesterone receptor
- Which one of the following statements regarding the prognosis of EMPD is true?
- Local recurrence after excision is common
- Local recurrence after excision is very rare
- Primary and secondary EMPD have similar survival rates
- Primary EMPD is characterized by a high mortality rate
- Secondary EMPD is characterized by a relatively good prognosis
References
- Battles OE, Page DL, Johnson JE. Cytokeratins, CEA, and mucin histochemistry in the diagnosis and characterization of extramammary Paget disease. Am J Clin Pathol. 1997;108(1):6-12.
- Caliskan M, Gatti G, Sosnovskikh I, et al. Paget disease of the breast: the experience of the European institute of oncology and review of the literature. Breast Cancer Res Treat. 2008;112(3):513-521.v
- Hammer A, Hager H, Steiniche T. Prostate-specific antigen-positive extramammary Paget disease--association with prostate cancer. APMIS. 2008;116(1):81-88.
- Hilliard NJ, Huang C, Andea A. Pigmented extramammary Paget disease of the axilla mimicking melanoma: case report and review of the literature. J Cutan Pathol. 2009;36(9):995-1000.
- Ivan D, Lazar A, Calonje E. Cutaneous metastases and Paget disease of the skin. In: Calonje JE et al., eds. McKee's Pathology of the Skin, 4th ed. Elsevier;2011:1257-1259.
- Kuan SF, Montag AG, Hat J, Krausz T, Recant W. Differential expression of mucin genes in mammary and extramammary Paget disease. Am J Surg Pathol, 2001;25(12):1469-1477.
- Regauer, S., Extramammary Paget disease—a proliferation of adnexal origin? Histopathology. 2006:48(6):723-729.
- Weedon D. Tumors of cutaneous appendages. In: Weedon D, ed. Weedon's Skin Pathology. Philadelphia, PA: Churchill Livingstone Elsevier; 2010:788-790.
Author
2013
Aleodor A. Andea, MD, MBA
Surgical Pathology Committee
University of Michigan
Ann Arbor, MI
Answer Key
- EMPD usually presents as a primary epidermal neoplasm without an associated carcinoma (c).
- Androgen receptor (a).
- Local recurrence after excision is common (a).