Clinical Summary
A 19-year-old woman presents with vaginal bleeding during the 14th week of pregnancy. She reports intractable nausea. Serum beta-human chorionic gonadotropin (beta HCG) levels are markedly elevated at 1,780,000 mIU/ml. Ultrasound assessment reveals no visible fetus, but a “snowstorm” pattern is noted by the radiologist. Curettage reveals 510 grams of bloody granular and friable tissue with numerous small vesicles, which contain clear colorless fluid. No fetal parts are seen grossly.
Master List of Diagnoses
- Choriocarcioma
- Gestational trophoblastic disease, complete molar type
- Gestational trophoblastic disease, partial molar type
- Hydropic abortus
- Invasive hydatidiform mole
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2016, case 23, and is gestational trophoblastic disease, complete molar type.
Criteria for Diagnosis and Comments
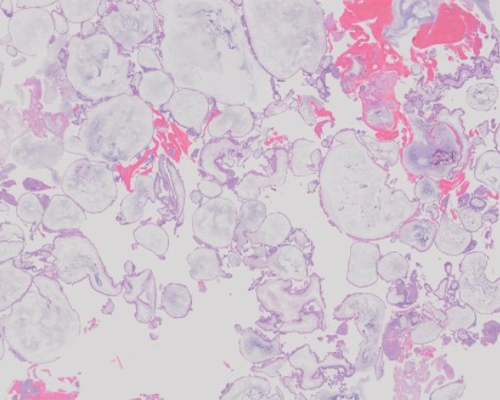
Microscopic sections reveal markedly edematous, round and bulbous chorionic villi. The intervillous stroma is also edematous. Trophoblastic hyperplasia is circumferential and focally is prominent, with occasional nuclear atypia and mitotic activity. Cisterns, acellular, fluid-filled spaces within a villus, demarcated by villus stroma, are common. The villi are either avascular or contain atrophic and/or dysmorphic vascular elements. Trophoblastic inclusions, invaginations cut en-face, may be seen in rare villi, but are uncommon. No convincing fetal parts are noted. The histologic features are most consistent with gestational trophoblastic disease (GTD), complete molar (CM) type. Classical GTD-CM presents in late first or early second trimester of pregnancy (8-18 weeks) with vaginal bleeding and an enlarged uterus for dates. Patients often present with intractable nausea and vomiting (hyperemesis gravidarum). Pulmonary emboli, pre-eclampsia, and hyperthyroid function are all potential complications. Gross findings include a large volume of hemorrhagic spongy tissue for a curettage (often over 500 grams), and prominent “grape-like” vesicles in clusters which ooze clear fluid.
Partial moles (GTD-PM) may resemble CM on gross exam but vesicles are less common or prominent, and the volume of tissue is still high. Patients usually present with a missed abortion at 8-22 weeks, and the beta HCG level is typically within normal limits or slightly increased. The uterus is not typically enlarged. The classic PM shows a bi-phasic population of enlarged and smaller villi, with the larger ones manifesting edematous villi with circumferential trophoblastic hyperplasia. In contradistinction with CM, trophoblastic inclusions are much more common and appear as cavities or invaginations in the villus stroma. These larger villi are more typically vascular and contain fetal nucleated red blood cells. Cistern formation occurs but is less prominent. The second villus population is relatively smaller and appears atrophic and/or fibrotic. GTD-PM specimens often include embryonic mesenchymal or visceral elements. Distinction between CM and PM in later gestations is relatively straightforward, but with the burgeoning use of ultrasound early in pregnancy, GTD is often clinically identified much earlier (6-8 weeks) and classification becomes more difficult with immature villi. Overlap in histologic features between CM and PM is not uncommon in these earlier cases. Cytogenetic assessment (and immunostaining with p57KIP2) may be helpful in diagnosis (discussed below).
The hydropic abortus (HA) yields substantially less tissue on curettage and presents as a missed or spontaneous abortion, typically at 6-14 weeks gestation. Beta HCG is not elevated, and the uterine size is either normal or low for dates. Microscopic evaluation reveals edematous but vascularized villi that have a smooth rounded contour. Trophoblastic hyperplasia, if present, is polar and not circumferential and trophoblastic inclusions are rare and typically completely absent. Embryonic elements are typically absent. Degenerative or autolytic foci may be present.
Cytogenetic analyses reveal that the typical GTD-CM has an androgenetic, diploid 46,XX karyotype (90%); the CM lacks maternal DNA. The remaining 10% are 46,XY and androgenetic but deriving from dispermy, ie, two sperm fertilizing an “empty” ovum lacking maternal chromosomes. GTD-PM is classically triploid, with two sets of paternal chromosomes (diandric) and one haploid maternal set, with the most common composition being 69,XXY, more rarely XXX, with XYY being the least common. Genetic aberrations have been reported in both CM and PM, however, with rare CM appearing triploid and PM appearing diploid; haploid, tetraploid, and aneuploid variants have all been reported. Some early moles may resist classification on purely histologic grounds.
Immunoevalution for p57KIP2, a cell cycle inhibitor, is expressed in the maternal allele in most tissues. Because CM contain only paternally derived genes, p57KIP2 is under-expressed or absent and immunoevaluation for the antigen shows absent or weak expression only in cytotrophoblast and villus stroma of GTD-CM. Cytotrophoblast and stroma of GTD- PM or HA, with a maternal genetic contribution, will show strong p57KIP2 expression and this can prove useful in confirming the diagnosis of GTD-CM (weak or absent expression) versus GTD-PM (strong expression). However, maternally derived, decidualized stromal cells will react strongly with the antibody and intervillous trophoblast islands in GTD-CM have been shown to express p57KIP2 and may cause confusion in interpretation. Thus, as with all immunostains, the expression pattern should be interpreted in context with other histologic and cytogenetic results, and its expression or absence should not be relied upon, alone, to classify GTD.
Repeat curettage after uterine evacuation of GTD may be performed if serum beta HCG levels do not decline, or if bleeding persists. The specimen is typically less voluminous and may reveal persistent GTD, choriocarcinoma, or simply a retained implantation site. A diagnosis of persistent GTD is rendered if residual atypical villi are found. If abundant trophoblasts without villi are seen, showing syncytiotrophoblast and cytotrophoblastic elements, a diagnosis of choriocarcinoma is rendered, especially if there is evidence of destructive myometrial invasion and necrosis. The prognosis of GTD overall is generally good in patients with no residual disease. Patients with GTD-PM have a very low risk of persistent disease (<1%). Patients with GTD-CM have a 10-20% risk of persistent disease and are typically followed carefully for 6-12 months to ensure beta HCG levels remain low. The risk of subsequent choriocarcinoma in GTD-CM is 3-5% in the US.
Choriocarcinoma is a malignant trophoblastic neoplasm and may arise subsequent to any gestation, including normal pregnancy. However, the risk is substantially greater with abnormal gestations (GTD), with GTD-CM being the most common antecedent diagnosis, present in roughly 50% of patients with choriocarcinoma. It should be in the differential diagnosis in any postpartum patient who presents with persistent bleeding and elevated beta HCG. The diagnostic findings include a dimorphic population of trophoblastic cells and absence of villi, typically with necrosis and hemorrhage. The dimorphic trophoblastic population includes multinucleated (and vacuolated) syncytiotrophoblastic cells admixed with mononuclear cytotrophoblastic or intermediate trophoblastic cells. These often have “plexiform” appearance on routine sections. It is vital to ensure that no villi are present, as the proliferative trophoblast in GTD-CM may closely mimic choriocarcinoma, and histologic sections should be carefully evaluated. The presence of necrosis and hemorrhage are also helpful clues in limited samples. Immunostains for CK-18 and inhibin are diffusely positive while p63, HPL, beta HCG, and CD-146 are focally to diffusely positive. While choriocarcinoma notoriously metastasizes widely to lung and brain, its former dismal prognosis has been reversed by cytotoxic chemotherapeutic regimens, and long-term survival now approaches 100%.
Invasive mole is diagnosed if there is histologic evidence of myometrial invasion by villi and hyperplastic trophoblast or if there is evidence of distant invasion such as elsewhere in the gynecologic tract (vagina, vulva) or remote sites (lung) by villi and trophoblast. Since there must be unequivocal evidence of myometrial invasion by abnormal villi and trophoblast, a definitive diagnosis of invasive mole by curettage alone is extremely difficult, and the diagnosis usually is made based on biopsy diagnosis of distant metastases, or by hysterectomy.
| Feature | GTD Complete Mole | GTD Partial Mole | Hydropic Abortus |
|---|---|---|---|
| Edema (“hydrops”) | Yes, prominent, grossly visible | Yes, variable; some may be grossly visible | Microscopic only, focal |
| Villous shape | Round or bulbous | Irregular, scalloped, biphasic population | Round, small |
| Cisterns | Yes, common | Variable | Typically absent |
| Trophoblastic inclusions | Rare | Common | Typically absent |
| Fetal/embryonic elements | Rare | Common | Typically absent |
| Trophoblastic distribution | Circumferential; multifocal | Circumferential; multifocal | Polar |
| Trophoblast proliferation | Common, often prominent | Present but less prominent | Rare |
| Trophoblast atypia | Present | Minimal | Absent |
| Implantation site | Exaggerated | Normal or exaggerated | Normal |
| Cytogenetics | 46,XX (paternal) | 69,XXY or XXX 2:1 paternal:maternal | Variable, often abnormal |
Supplementary Questions
- Which of following is the most common cytogenetic pattern seen in gestational trophoblastic disease, complete mole?
- 46,XX (androgenetic)
- 46,XX (gynegenetic)
- 69,XXX
- 69,XXY
- Aneuploidy
- Which of the following histologic findings are more typical in gestational trophoblastic disease, partial mole?
- A biphasic population of villi with larger forms showing circumferential hyperplasia and trophoblastic inclusions, and smaller atrophic and fibrotic villi
- A single population of bulbous villi with prominent circumferential trophoblastic hyperplasia
- Absence of embryonic mesenchymal or visceral remnants
- Prominent, voluminous cistern formation and “grape-like” clusters on gross exam
- Scanty amounts of tissue on curettage
- Which of the following diagnostic finding(s) is/are essential for the diagnosis of invasive mole versus choriocarcinoma?
- Persistently elevated beta HCG after uterine evacuation of gestational trophoblastic disease
- The finding of a 46,XXX androgenetic genotype
- The presence of a biphasic population of trophoblastic cells
- The presence of atypical villi and trophoblast with unequivocal myometrial invasion
- The presence of cistern formation in villi
References
- Nucci MR, Oliva E. Gynecologic Pathology. New York, NY: Churchill Livingstone Elsevier; 2009:645-665.
- Mazur, MT, Kurman RJ. Diagnosis of Endometrial Biopsies and Curettings. 2nd Ed. New York, NY: Springer; 2005:67-94.
- Shih I, Mazur MT, Kurman, RJ. Gestational trophoblastic tumors and related tumor–like lesions, chapter 20 in Kurman, RJ, Ellenson, LH, Ronnett, BM, eds. Blaustein's Pathology of the Female Genital Tract. 6th Ed. New York, NY: Springer; 2011:1090-1101.
Author
2016
Philip A Branton MD
Surgical Pathology Committee
Biorepositories and Biospecimens Research Branch
National Cancer Institute
Rockville, MD
Answer Key
- 46,XX (androgenetic) (a)
- A biphasic population of villi with larger forms showing circumferential hyperplasia and trophoblastic inclusions, and smaller atrophic and fibrotic villi (a)
- The presence of atypical villi and trophoblast with unequivocal myometrial invasion (d)