- Home
- Member Resources
- Pathology Case Challenge
- Thyroid Gland, Left Lobe
Clinical Summary
A 40-year-old woman presents with left neck swelling, stridor, and dysphagia. Physical examination reveals a left neck mass. The patient is euthyroid and thyroid function tests are within normal limits. She has no family history of thyroid disorders and no history of head and neck radiation. Computed tomography shows tracheal compression and numerous thyroid nodules in the left thyroid lobe; the right thyroid lobe is unremarkable. A fine needle aspiration (FNA) of the left thyroid lobe is interpreted as “follicular lesion of undetermined significance.” Left thyroid lobectomy is performed. A 60 g thyroid lobectomy shows numerous vague glistening nodules, 1.1 to 4.5 cm, with semitranslucent content, involving the entire lobe. Rare incomplete fibrous strands partially surround some of the nodules. Only a thin rim of unremarkable thyroid tissue is identified at the periphery of the lobe.
Master List
- Diffuse toxic hyperplasia (Graves disease)
- Dyshormonogenetic goiter
- Follicular adenoma
- Nodular thyroid hyperplasia (multinodular goiter)
- Papillary thyroid carcinoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2014, case 01, and is nodular thyroid hyperplasia (multinodular goiter)
Criteria for Diagnosis and Comments
Practically, the first challenging aspect of this case is gross examination and selection of tissue sections for microscopic examination. In this case, a multinodular process distorts the contour of the lobe and, in general, surgeon's suture marking the superior or inferior pole may be the only clue for orientation. An additional potential landmark may be the cauterized isthmic surface (indicating inferior pole). In the presence of a dominant nodule, correlation with preoperative imaging studies may be used to orient the lobectomy, too. Parenthetically, most lymph nodes in thyroid lobectomy specimens are identified by submitting isthmic fibroadipose tissue. The parathyroid glands are easier to find before the specimen is inked.
Grossly, the entire lobe is spongy and diffusely involved by numerous vague coalescing brown nodules, some with microcystic changes, separated by irregular fibrous strands of variable thickness (about 0.1 cm). While the contour of the lobe is distorted, all nodules are confined to the lobe. None of the nodules are completely surrounded by fibrous strands; therefore, true encapsulation is absent. Most nodules are filled with abundant translucent yellow colloid. There is no evidence of calcification or of distinct infiltrative solid white-gray areas.
Evidence–based studies of thyroid sampling are exceptionally rare and focus mostly on encapsulated lesions. In this case, since no distinct encapsulated lesions are noted and the nodular process is affecting the entire lobe, 1 tissue section per 5.0-10.0 g of thyroid tissue (perhaps up to 10 sections/lobe) or 1 tissue section per largest nodule (up to 5 nodules) will most likely satisfy the informal minimal standard. When an encapsulated nodule is identified, at least 10 sections of the capsule or, ideally, the entire capsule has to be examined microscopically for the presence of capsular or vascular invasion.
In cases with tan fleshy areas (resembling cut surface of lymph nodes), additional sampling may be warranted to address the possibility of lymphoma. The clinical significance of identifying indolent and incidental foci of papillary thyroid microcarcinoma is uncertain. However, in cases with metastatic papillary thyroid carcinoma (PTC) identified in cervical lymph nodes dissected for an unrelated condition (eg, squamous cell carcinoma of the head and neck) and without grossly identifiable focus of primary PTC, initial sampling of the normal thyroid tissue may be of highest yield.
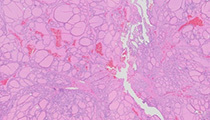
Microscopically, the left thyroid lobe is characterized by follicles of variable size and shape. The larger follicles are comprised of flattened follicular cells, while taller, columnar follicular cells line the smaller follicles. The colloid thickness varies from thin in larger follicles to slightly thicker in smaller follicles. Focal colloid scalloping is seen. Some foci are characterized by nonbranching papillary projections with thin fibrovascular cores and "follicle-in-follicle" arrangements. In this case, very few tissue sections show clear cell change or oncocytic metaplasia. Degenerative changes (eg, hemorrhage) are minimal.
Although the term "goiter" is commonly used in surgical pathology reports, the histopathologic changes are perhaps more appropriately described as "nodular hyperplasia." While clinically "goiter" simply indicates thyroid enlargement, there are no clear cut-off weight or size values to be used by pathologists to objectively diagnose thyroid enlargement (especially since both weight and size of thyroid glands may vary with patient's weight, gender, age, geography, and various physiologic states [eg, pregnancy, puberty]).
Endemic (secondary to dietary iodine deficiency) and sporadic nodular thyroid hyperplasia have similar histopathologic presentation. Sporadic multinodular goiter may be caused by a variety of medications that interfere with thyroid hormone synthesis, including lithium, thalidomide, iodine, and amiodarone. While minocycline appears to inhibit thyroid peroxidase, it induces black pigmentation of the thyroid gland, most commonly without the enlargement of the thyroid gland.
Cytologically, the follicular cells in this case are characterized by minimal chromatin clearing, basally oriented nuclei, and less than 2-fold nuclear enlargement. Before accepting nuclear enlargement or crowding as worrisome for PTC, it is important to remember that cytologic alterations are scattered throughout the gland, between numerous vague nodules and do not form a distinct lesion.
Special studies may be helpful in further excluding the possibility of PTC. Immunostains for HBME-1 and galectin-3 are usually negative in thyroid hyperplasia. However, HBME-1 may highlight solid cell nests, parathyroid tissue, red blood cells in the areas of FNA needle track, and show apical membranous staining in a subset of follicular cells with hyperplastic change. Of note, in most cases of PTC, HBME-1 stains lateral/intercellular membranes, also. Galectin-3 should be interpreted as positive only when both cytoplasmic and nuclear staining are present (galectin-3 will highlight histiocytes and giant cells, a helpful positive internal control).
It is still unclear whether distinct nodules in the background of nodular goiter are hyperplastic or neoplastic in nature. Practically, the differentiation of "follicular adenoma" from "hyperplastic nodule" is performed based on morphologic presentation alone. In our case, some tissue sections reveal more prominent /dominant hyperplastic nodules almost entirely encircled by fibrous strands. This appearance does raise the possibility of a follicular adenoma in the background of nodular thyroid hyperplasia. The presence of abundant colloid and of more than one growth pattern within the dominant nodule with combination of macro-, normo-, and microfollicles would argue in favor of a hyperplastic nodule. One way to assess the variability in the intranodular growth pattern is to compare it to the adjacent normal thyroid. A similar appearance of the thyroid tissue within and outside of the nodule (or on both sides of the presumed capsule/rim of fibrous tissue) and the lack of compression changes in the adjacent thyroid would be most consistent with a hyperplastic nodule. One of the possible practical implications of confusing hyperplastic nodule with a follicular adenoma, would be the under-sampling of the capsule of the nodule. Therefore, additional sections of the capsule or of nodule/adjacent normal thyroid interface can be submitted for microscopic examination, when the concern for follicular adenoma persists and if institutional grossing standards call for the examination of the entire capsule in cases of follicular adenoma.
Most cases of dyshormonogenetic goiter are autosomal recessive disorders associated with congenital hypothyroidism and are clinically apparent before the age of 25.
Clinically, euthyroid status and asymmetric involvement of only one lobe refute the possibility of diffuse toxic hyperplasia (Graves disease), an autoimmune disorder. Histologically, in cases of diffuse toxic hyperplasia, the colloid is more scant and thinner, colloid scalloping is more prominent, and follicular hyperplasia is not limited to nodules.
Supplementary Questions:
- Which of the following types of thyroid disorders is an autosomal recessive disorder?
- Diffuse toxic hyperplasia (Graves disease)
- Dyshormonogenetic goiter
- Endemic goiter
- Nodular thyroid hyperplasia
- Papillary thyroid carcinoma
- Submission of the entire capsule of a nodule for microscopic evaluation (as opposed to 1 section/1.0 cm of the nodule) appears to increase the chance of identifying foci of vascular and/or capsular invasion.
- True
- False
- Which of the following medications is not associated with multinodular goiter?
- Amiodarone
- Iodine
- Lithium
- Minocycline
- Thalidomide
References
- Biddinger PW. Diffuse and nodular hyperplasia. In: Nikiforov Y, Biddinger PW, Thompson LDR, eds. Diagnostic Pathology and Molecular Genetics of the Thyroid. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2012:69-93.
- Seethala R, Nikiforov Y. Gross examination. In: Nikiforov Y, Biddinger PW, Thompson LDR, eds. Diagnostic Pathology and Molecular Genetics of the Thyroid. 2nd ed. Philadelphia, PA: Lippencott Williams & Wilkins; 2012:403-409.
- Yamashina M. Follicular neoplasms of the thyroid. Total circumferential evaluation of the fibrous capsule. Am J Surg Pathol.1992;16(4):392–400.
Authors
2014
Simion I. Chiosea, MD
Surgical Pathology Committee
University of Pittsburgh Medical Center
Pittsburgh, PA
Answer Key
- Dyshormonogenetic goiter (b).
- True (a).
- Minocycline (d).