- Home
- Member Resources
- Pathology Case Challenge
- Third Trimester Placenta
Clinical Summary
A 22-year-old G2P1 woman is admitted in labor via the emergency room (ER) to a local hospital. She informs the admitting physician that based on prior ultrasound evaluations her fetus exhibits findings consistent with intrauterine growth restriction and that she regularly visits the hospital’s obstetrical service, where she is being followed by a staff gynecologist. At the time of admission, she denies fever, cough, or skin rashes. Evaluation of her chart reveals that she is 37 weeks pregnant (by dates). Also noted are several pre-natal laboratory results, including the following: HBsAg-negative, RPR non-reactive, Rubella-immune, HIV non-reactive, GC-negative, and Chlamydia-negative. Due to fetal distress, she delivers via Cesarean-section later that day; the newborn male is small for gestational age. The placenta is submitted to the pathology department for evaluation.
Master List:
- Basal villitis
- Chronic chorioamnionitis
- Chronic deciduitis
- Chronic histiocytic intervillositis
- Chronic villitis of unknown etiology
- Cytomegalovirus, chronic placentitis
- Placental infarcts
- Syphilis, chronic placentitis
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2015, case 23 and is chronic villitis of unknown etiology.
Criteria for Diagnosis and Comments
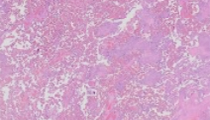
The placenta is determined to be small for gestational age based on its weight and the ratio between the weight of the newborn and the weight of the placenta. No gross abnormalities of the umbilical cord or fetal membranes are noted. However, serial sectioning of the disc reveals irregular areas of pale discoloration and consolidation. No distinct areas of infarction are identified. Microscopic evaluation reveals an extensive chronic inflammatory process with diffuse involvement of all representative placental tissue sections. The inflamed chorionic villi are arranged in clusters that vary from less than 3 villi to a predominant pattern consisting of more than 10 villi (many clusters arranged in a confluent pattern). These inflamed villous clusters alternate with late third trimester non-inflamed villi. The inflammatory infiltrate varies from mild to marked, and consists of lymphocytes and histiocytes; in scattered areas there are occasional neutrophils. Rare multinucleated giant cells are focally noted. Although the inflammation mostly involves the villous stroma, it extends significantly into the intervillous space. Perivillous fibrin deposition is also prominently noted in association with these inflamed villous clusters, especially the larger ones. In some foci the inflamed villi are fibrotic and avascular. Obliterative fetal vasculopathy with vascular occlusion is noted in many areas. The chronic inflammatory process focally involves the subchorionic fibrin and extends into the mostly fibrosed chorionic plate, variably involving the chorion and amnion; a minor component of neutrophils is also noted in some areas. Many chorionic plate vessels are also inflamed. The chronic inflammatory process extends into the basal villi. The decidua exhibits areas of necrosis and involvement by lymphocytes and plasma cells, occasionally mixed with neutrophils; this inflammatory pattern is consistent with chronic deciduitis. The uninvolved third trimester villi are prominently congested and very focally exhibit delayed maturation. Scattered microcalcifications are noted. Areas of increased fibrin deposition also reveal occasional embedded necrotic villi. The extraplacental fetal membranes are fibrosed and involved by lymphocytes and histiocytes (in a manner similar to the chorionic plate); this pattern is consistent with chronic chorioamnionitis. There is no evidence of acute chorioamnionitis or funisitis. Fetal and placental viral and bacterial tissue cultures are negative. The inflammatory histological findings identified in this case are consistent with a diagnosis of third trimester placenta with diffuse chronic villitis of unknown etiology (VUE).
Incidence: Chronic villitis of unknown etiology (also known as non-specific chronic villitis, idiopathic villitis, and non-infectious chronic villitis) can be seen in 5 to 15% of placentas, usually near or at term. On the other hand, infectious chronic villitis (usually caused by the TORCH organisms), affects between 0.1 and 0.4 % of placentas, usually in the late second/early third trimester.
Etiology: Although studies suggesting that VUE is caused by infectious agents exist in the literature, there are numerous investigators that challenge the “infectious origin” hypothesis. Some studies suggest that VUE is the result of placental infection by a yet to be discovered microorganism or by some known bacteria or virus that eludes detection by current testing methodologies. However, it is not uncommon for mothers and infants with placentas involved by VUE to lack the classic clinical signs and symptoms of infectious conditions, as well as positive serological tests and/or positive bacterial or viral cultures. The absence of seasonal variations in the incidence of VUE, combined with the absence of specific geographic patterns of occurrence, also discount the “infectious origin” hypothesis. Many studies support the hypothesis that VUE represents an “immune response” of maternal origin occurring within fetal tissue (an immunological response similar to a "host-versus-graft" process). Findings that favor this “immune response” hypothesis include the presence of CD8+ predominant maternal T-cells (maternal CD68+ histiocytes and CD4+ T-cells also occur, and a few B cells and NK cells can also be present) and antigen presenting Hofbauer cells (fetal histiocytes) in the inflamed villous areas. Studies indicating the maternal immune recognition of fetal antigens in this setting include those demonstrating activation of histocompatibility antigens and activation of the normally repressed JAK-STAT-1 pathway mediated by gamma interferon and CD4+ T-cells. A recent study reported an association between VUE and positive C4d complement staining villous syncytiotrophoblast; C4d staining was observed in both chronically inflamed and nearby non-inflamed chorionic villi. Additional studies are necessary to further elucidate the nature of this entity, including why if VUE is the result of a maternal immunological rejection process it only occurs in a relatively small number of cases.
Clinical features: Intrauterine growth restriction is the most common condition associated with VUE. Of importance is the fact that VUE may recur in subsequent pregnancies, with recurrence rates between 10% and 25 % reported in the literature. Cases of recurrent VUE are more commonly associated with maternal infertility, recurrent miscarriages, and maternal autoimmune diseases. VUE can be identified in placentas from cases of intrauterine fetal demise, recurrent miscarriages, prematurity, abnormal neurological development, and cerebral palsy (among other conditions). However, most placentas exhibiting VUE are from cases in which a healthy baby is delivered. In twin gestations one or both placentas may be affected by VUE and if both placentas are involved, the degree of involvement may be similar or different (this may result in discordant twin size). Non-specific basal chronic villitis (basal villitis, see below) may recur in subsequent pregnancies. Recurrent basal villitis is more commonly associated with recurrent pelvic infections than with autoimmune conditions or infertility; it is more commonly noted in placentas from premature infants than VUE.
Gross and microscopic findings: Placentas involved by VUE are often small for gestational age. When placentas are severely involved by VUE they may exhibit irregular pale discoloration and consolidation of the involved parenchymal areas. According to the literature, about 90% of VUE cases are detected with a standard placental disc sampling of 2 to 3 sections, with the detection rate reaching its maximum at 4 sections. The placental involvement by VUE varies from focal to diffuse, but even in the diffuse pattern not all villi are involved. There are several histological patterns that can be observed in these placentas, and some authors report a correlation between the degree of villous involvement and fetal outcome. In the most common pattern (close to 50% of all cases) the chronic inflammation involves terminal and mature intermediate villi (distal villi). In close to one third of cases, the chronic inflammation involves the proximal stem villi in addition to the distal villi; the chorionic plate may also be involved in this setting. According to the literature, this pattern can be seen in association with obliterative fetal vasculopathy, resulting in areas of avascular villi formation (that may be extensive). In the least common pattern (close to 20% of cases) the anchoring villi of the basal plate and the adjacent terminal villi are involved by the chronic inflammatory process (basal villitis). Although decidual lymphoplasmacytic inflammation is commonly associated with basal villitis, it can also be seen in association with the other two patterns. Chronic chorioamnionitis, perivillous fibrin deposition, and villous fibrosis can also be seen in association with VUE. However, VUE is not commonly associated with acute inflammation of the umbilical cord, fetal membranes, and/or the chorionic plate.
Differential diagnosis: Several infectious agents can cause chronic placentitis. Included in this list are the TORCH organisms (Toxoplasma gondii, Rubella, Cytomegalovirus (CMV), and Herpes simplex), Treponema pallidum, varicella-zoster virus, Epstein-Barr virus, and Trypanosoma cruzi. In these cases, the chronic villous inflammation is diffuse, and commonly associated with funisitis, chorioamnionitis, and/or deciduitis. In many situations the clinical history of the mother and/or the baby as well as the results of serological tests and/or tissue cultures can assist in determining the infectious etiology of the chronic placentitis. The microscopic features characteristic of many of these infections can assist in excluding placental involvement by VUE. For example, in cases of congenital syphilis the more “classic” placental microscopic findings include a diffuse histiocytic predominant villitis, proliferative endovasculitis, and necrotizing umbilical periphlebitis; spirochetes can be demonstrated (especially in the infected umbilical cord) with the use of special histochemical stains. In cases of congenital CMV placentitis the more “classic” microscopic findings include a diffuse and prominent villous fibrosis and mineralization, prominent plasma cell infiltrates in the villous stroma and the presence of large intranuclear inclusions with or without smaller basophilic cytoplasmic inclusions; immunohistochemistry staining for CMV can assist in highlighting the presence of infected cells. Nevertheless, some cases of VUE may raise the question of an infectious process (e.g., those with numerous multinucleated giant cells and/or non-caseating granulomas). Special studies (e.g., histochemical stains, immunohistochemical stains) may then be indicated to completely exclude an infectious etiology.
There are other considerations in the differential diagnosis of VUE. Chronically inflamed chorionic villi (sometimes associated with a perivillous inflammatory component) are commonly noted at the periphery of placental infarcts. If infarcts were described upon gross evaluation of the placenta, be sure that the apparent “focal chronic villitis” does not represent the edge of an infarct. In these cases, deeper tissue sections or additional representative tissue sections may assist in clarifying the association of the chronic villous inflammatory process with the infarct. Perivillous chronic inflammation (sometimes very prominent) is not uncommon in cases of VUE. However, when the inflammation is confined to the perivillous space (without villous involvement) VUE is excluded. Conditions such as chronic histiocytic intervillositis (massive chronic intervillositis) need to be considered in this setting.
Supplementary Questions:
- Which of the following is the most common condition associated with chronic villitis of unknown etiology?
- Delivery of an infant with cerebral palsy
- Intrauterine fetal demise
- Intrauterine growth restriction
- Meconium aspiration syndrome
- Recurrent spontaneous abortion
- In close to one-third of cases of chronic villitis of unknown etiology, the chronic inflammation involves the proximal stem villi, in addition to the distal villi; the chorionic plate may also be involved in this setting. According to the literature, which of the following can be associated with this pattern?
- Fetal thrombotic vasculopathy
- Hypertrophic decidual vasculopathy.
- Necrotizing umbilical periphlebitis
- Obliterative fetal vasculopathy
- Proliferative endovasculitis
- Chronic villitis of unknown etiology may recur in subsequent pregnancies, with rates between 10% and 25% reported in the literature. With which of the following are cases of recurrent chronic villitis of unknown etiology most commonly associated?
- First pregnancy before the age of 20
- History of prior voluntary interruption of pregnancy
- Maternal age > 35 years old and multiparity
- Maternal infertility, recurrent miscarriages, and maternal autoimmune diseases.
- Recurrent pelvic infections
References
- Jacques SM, Qureshi F. Chronic villitis of unknown etiology in twin gestations. Pediatr Pathol. 1994;14:575-584.
- Katzman PJ, Murphy SP, Oble DA. Immunohistochemical analysis reveals an influx of regulatory T cells and focal trophoblastic STAT-1 phosphorylation in chronic villitis of unknown etiology. Pediatr Dev Pathol. 2011;14:284-293.
- Kim JS, Romero R, Kim MR, Friel L, Espinoza J, Kim CJ. Involvement of Hofbauer cells and maternal T cells in villitis of unknown aetiology. Histopathology. 2008;52:457-464.
- Knox WF, Fox H. Villitis of unknown aetiology: its incidence and significance in placentae from a British population. Placenta. 1984;5:395-402.
- Kraus FT, Redline RW, Gersell DJ, Nelson DM, Dicke JM. Chapter 5: Inflammation and Infection. AFIP Atlas of Nontumor Pathology, First Series, Fascicle 3: Placental Pathology. Washington, DC. American Registry of Pathology;2004:75-115.
- Myerson D, Parkin RK, Benirschke K, Tschetter CN, Hyde SR. The pathogenesis of villitis of unknown etiology: analysis with a new conjoint immunohistochemistry-in situ hybridization procedure to identify specific maternal and fetal cells. Pediatr Dev Pathol. 2006;9:257-265.
- Redline RW, Pappin A. Fetal thrombotic vasculopathy: the clinical significance of extensive avascular villi. Hum Pathol. 1995;26:80-85.
- Redline RW. Villitis of unknown etiology: noninfectious chronic villitis in the placenta. Hum Pathol. 2007; 38:1439-1446.
- Rudzinski E, Gilroy M, Morgan T, Newbill C, Rudzinski E. Morgan T. Positive C4d immunostaining of placental villous syncytiotrophoblsts supports host-versus-graft rejection in villitis of unknown etiology. Pediatr Dev Pathol. 2013;16:7-13.
Author
Nilsa C. Ramirez, MD
Surgical Pathology Committee
Nationwide Children’s Hospital
Columbus, OH
Answer Key
- Intrauterine growth restriction (c)
- Obliterative fetal vasculopathy (d)
- Maternal infertility, recurrent miscarriages, and maternal autoimmune diseases (d)