A 35-year-old Caucasian man presents to his physician complaining of a painless right testicular mass that has been growing over the last 3 months. Laboratory testing reveals elevated alpha-fetoprotein (AFP) and human chorionic gonadotropin (HCG). Ultrasound shows a multicystic lesion of the right testis that measures 7.0 cm in greatest dimension. Cut section reveals a 7.0 cm mass with cystic areas, and a gray-tan cut surface hemorrhagic and/or necrotic foci. A radical orchiectomy is performed.
Master List
- Embryonal carcinoma
- Mature teratoma
- Mixed germ cell tumor
- Seminoma
- Yolk sac tumor
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2016, case 02, and is mixed germ cell tumor
Criteria for Diagnosis and Comments
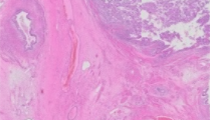
Sections of the lesion contain several distinct components, the largest of which includes cysts lined by keratinizing squamous epithelium and cystic structures lined by glandular epithelium. Also seen are immature cartilage, primitive mesenchyme, and neuroectodermal tissue. These findings represent both mature and immature teratoma. Other areas show collections of cells with overlapping, large, pleomorphic, and hyperchromatic nuclei with prominent nucleoli and areas of necrosis and hemorrhage representing embryonal carcinoma. Yolk sac tumor with a glandular/alveolar pattern with rare hyaline globules is present. Nests of syncytiotrophoblasts are present with some of these nests appearing to be associated with cytotrophoblasts indicating a small component of choriocarcinoma. No seminomatous component is identified. These features are consistent with a diagnosis of mixed germ cell tumor. The distributed slides all contain teratoma and at least one other component.
Mixed germ cell tumors (GCTs) contain two or more germ cell tumor types present within a single mass. This entity is the second most common germ cell tumor in adults, after seminoma, comprising 30-50% of cases. Any combination of teratoma, embryonal carcinoma, yolk sac tumor, choriocarcinoma, and seminoma can be seen. These tumors typically occur in adults aged 20-50 years, with an average age at diagnosis of 30 years. Of note, however, tumors that contain seminomatous elements tend to occur at a later age than those without a seminomatous component. Mixed GCTs are more common in Caucasian individuals and rarely occur in prepubescent children. Presenting symptoms may include testicular enlargement with or without pain and some patients may present with signs and symptoms associated with metastases. Serum elevation of AFP and HCG can be seen, corresponding to the presence of yolk sac tumor elements and choriocarcinoma, respectively. Ultrasound may be useful for evaluation and can reveal a heterogenous echotexture, irregular margins, cystic components, and echogenic foci that represent areas of hemorrhage and calcification. The exact findings can differ depending on the composition of the tumor. Imaging studies are also used to identify lymph node involvement, particularly retroperitoneal lymph nodes, and distant metastases.
Mixed GCTs often have a variegated cut surface, with solid, cystic, firm, soft, hemorrhagic, and/or necrotic areas, reflecting different combinations of neoplastic components. The most common histologic subtype seen is embryonal carcinoma, followed by teratoma, yolk sac tumor, seminoma, and choriocarcinoma. These subtypes are seen in varying proportions and are often irregularly-spaced throughout the tumor. The more common combinations seen include embryonal carcinoma and teratoma as well as embryonal carcinoma and seminoma. The histological appearances of these subtypes are similar to that of the pure forms of these tumors. For mixed GCTs, all components should be listed along with the approximate proportion of each component. The proportion of embryonal carcinoma is particularly important as its presence in >80% of the tumor is a predictor for metastatic disease in patients with clinical stage I mixed GCTs. Other poor prognostic indicators include a mediastinal primary (as opposed to testis or retroperitoneal primary), nonpulmonary visceral metastases, an AFP ≥10,000 ng/ml, an HCG ≥ 50,000 mIU/ml, or a lactate dehydrogenase (LDH) ≥ 10x the upper limit of normal, which is 333 IU/L.
Treatment of mixed GCTs is dependent on stage. Stage I disease is locally confined with no evidence of solid organ or lymphatic spread. Serum markers, if elevated, return to normal after orchiectomy. In fact, continued elevation of serum markers after orchiectomy indicates probable metastatic disease. Of patients with a clinical diagnosis of stage I disease, nearly 30% have microscopic metastases to retroperitoneal lymph nodes. This percentage is increased in patients with vascular or local invasion or >80% embryonal carcinoma component as determined by pathological examination. For this reason, stage I mixed GCTs may be treated with orchiectomy plus retroperitoneal lymph node dissection. Other treatment options for localized disease include aggressive surveillance consisting of regular office visits, tumor marker measurements, chest radiography, and abdominal and pelvic computed tomography (CT) scans. Stage II disease (metastatic disease to the retroperitoneal lymph nodes) is often managed with orchiectomy plus retroperitoneal lymph node dissection or chemotherapy. The risk of recurrence in stage II disease is increased if there is involvement of more than 5 nodes, if one or more of the involved nodes are larger than 2.0 cm, or if there is extranodal extension. Stage III (supradiaphragmatic lymph node or visceral involvement or persistently elevated markers) and bulky stage II disease are often treated with initial chemotherapy, followed by surgery. The presence of residual embryonal carcinoma necessitates additional chemotherapy.
It is important to distinguish mixed GCTs from a pure seminoma, as treatment for the latter is different. The pure seminoma often presents in the 4th decade of life, later than most other germ cell tumors, and is the most common germ cell tumor, comprising approximately 40% of all testicular germ cell tumors. Histologically, seminoma has a “fried egg” appearance with large, uniform, round and evenly-spaced nuclei, surrounded by abundant clear cytoplasm. These cells are usually arranged in sheets separated by fibrous bands containing lymphocytes. Around 10-20% of classic seminomas may contain syncytiotrophoblastic giant cells that can cause an elevation of serum HCG. The prognosis of seminomas with increased HCG is not altered. Immunohistochemistry is reactive for OCT3/4, PLAP, and KIT. Treatment is orchiectomy with possible radiotherapy.
Embryonal carcinoma is composed of cells with overlapping, large, pleomorphic, and hyperchromatic nuclei with prominent nucleoli. Numerous mitoses and bizarre forms are often seen. Patterns of growth seen include solid, syncytial, acinar, papillary, and tubular. A key feature of this tumor on low power is the presence of large areas of hemorrhage and necrosis. Embryonal carcinoma is most often seen in mixed tumors but can also be seen in its pure form. It is an aggressive tumor with approximately two thirds of cases presenting with lymph node or distant metastases. Immunohistochemistry is reactive for CD30, cytokeratins, OCT3/4, and PLAP, but nonreactive for KIT.
Teratomas are composed of tissue derived from the endoderm, mesoderm, and ectoderm, such as epithelium, cartilage, fat, bone, muscle, and neural elements. Well-differentiated tissues are referred to as mature, whereas embryonic or fetal-like tissues are referred to as immature. In prepubescent males, this tumor is benign and almost always presents in its pure form. In adults, the teratoma is usually present as a component of mixed GCTs and has metastatic potential. Of note, malignant transformation can occur in the elements present, including adenocarcinoma or squamous cell carcinoma. It is important to distinguish metastatic teratoma from primary carcinomas, as treatment and prognosis are different. Treatment of pure teratoma is often orchiectomy plus retroperitoneal lymph node dissection.
Yolk sac tumors are the most polymorphous of the germ cell tumors. Patterns include microcystic, macrocystic, solid, glandular/alveolar, endodermal sinus, papillary, hepatoid, and glandular arrangements. The microcystic pattern is the most common. Virtually all tumors demonstrate multiple patterns in varying proportions. Cytologically, the cells are small with pleomorphic nuclei and cleared cytoplasm. Intracytoplasmic, PAS-positive hyaline globules are consistently present. Interestingly, the stroma is also neoplastic and may serve as a stem cell reservoir. Immunohistochemistry is positive for keratin, OCT3/4, and usually AFP. Yolk sac tumors occur in both pre- and post-pubertal males and are the most common malignant germ cell tumor before puberty.
Supplementary Questions:
- Which of the following pure germ cell tumors is most important to distinguish from a mixed germ cell tumor?
- Choriocarcinoma
- Embryonal carcinoma
- Mature teratoma
- Seminoma
- Yolk sac tumor
- Which of the following is not a poor prognostic indicator for mixed germ cell tumors?
- AFP ≥10,000 ng/ml
- HCG ≥ 50,000 mIU/ml
- LDH ≥ 10x the upper limit of normal
- Mediastinal primary
- Pulmonary metastases
- Which histologic component, when present in >80% of the tumor, is a predictor for metastatic disease in stage I mixed germ cell tumors?
- Choriocarcinoma
- Embryonal carcinoma
- Immature teratoma
- Seminoma
- Yolk sac tumor
References
- Albers P, Albrecht W, Algaba F, et al. EAU Guidelines on testicular cancer: 2011 update. Eur Urol. 2011;60(2):304-319.
- Bahrami A, Ro JY, Ayala AG. An overview of testicular germ cell tumors. Arch Pathol Lab Med. 2007;131(8):1267-1280.
- Gori S, Porrozzi S, Roila F, Gatta G, De Giorgi U, Marangolo M. Germ cell tumours of the testis. Crit Rev Oncol Hematol. 2005;53(2):141-164.
- Mosharafa AA, Foster RS, Leibovich BC, et al. Histology in mixed germ cell tumors. Is there a favorite pairing? J Urol. 2004;171(4):1471-1473.
- Nallu A, Mannuel HD, Hussain A. Testicular germ cell tumors: biology and clinical update. Curr Opin Oncol. 2013;35(3):266-272.
- Ro JY, Dexeus FH, el Naggar A, Ayala AG. Testicular germ cell tumors: clinically relevant pathologic findings. Pathol Annu. 1991;26:59-87.
Authors
2016
Alex Feldman, MD
Pathology Resident
University of Alabama at Birmingham
Birmingham, AL
Thomas Winokur, MD
Surgical Pathology Committee
Associate Professor of Pathology
University of Alabama at Birmingham
Birmingham, AL
Answer Key
- Seminoma (d)
- Pulmonary metastases (e)
- Embryonal carcinoma (b)