Clinical Summary
A 92-year-old woman presents with abdominal fullness and epigastric pain. She reports a 40-pound weight loss over the past year. On computed tomography, a mass is identified involving the stomach. She undergoes a gastrectomy and partial omentectomy. An ulcerating 6.0 cm, mucosal-based mass is present along the entire circumference of the antrum and pyloric channel. The overlying serosa is fibrotic and the omentum is adherent. The resection specimen consists of the stomach mass.
Master List of Diagnoses
- Invasive micropapillary carcinoma of stomach
- Metastatic mucinous carcinoma of breast
- Metastatic mucinous carcinoma of lung
- Metastatic papillary carcinoma of bladder
- Mucinous adenocarcinoma of stomach
- Papillary adenocarcinoma of stomach
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2016, case 01, and is mucinous adenocarcinoma of stomach
Criteria for Diagnosis and Comments
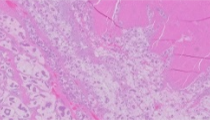
The H&E stained section reveals an infiltrative tumor located in the submucosa and muscularis propria, composed of epithelial tumor cells growing in clusters surrounded by mucin. The epithelial clusters are relatively uniform in size, lack fibrovascular cores, and exhibit poorly formed central lumens. The nuclei demonstrate moderate to marked pleomorphism, with prominent nucleoli and granular chromatin. The cytoplasm varies from granular and eosinophilic to slightly clear with occasional intra-cytoplasmic lumina. The cells are polarized, with the nuclei gravitating towards the perimeter of the clusters.
Immunohistochemical stains of the tumor cells show positivity for cytokeratin 7, CEA, cadherin 17, and CDX2. The neoplasm is negative for CK20, GATA-3, and TTF1. Overall, these are features of mucinous adenocarcinoma of gastric origin.
Mucinous adenocarcinomas of the stomach comprise one of the five main histologic types of gastric adenocarcinomas recognized by the WHO classification. This subtype represents approximately 10% of gastric cancers. These tumors are comprised of glands and clusters of cells floating in background mucin. By definition, gastric mucinous carcinomas show more than 50% extracellular mucin production.
Gastric carcinoma is a heterogeneous disease, in the population effected, the area of stomach involved, and in the histologic appearances. The risk of gastric carcinoma increases with age and is relatively rare in young individuals <30 years of age unless there is a hereditary component. Epidemiologic studies have shown varying rates of gastric cancers in the world, with the highest incidence in Eastern Europe, Eastern Asia, and South America. In these areas, the intestinal type involving the antrum and pylorus predominates. The lowest rates of gastric carcinoma are seen in North America, Northern Europe, Southeast Asia and Africa where the diffuse type involving the cardia is most frequent.
Helicobacter pylori (H. pylori) infection has been shown to be the most important cause of distal gastric adenocarcinoma. It is postulated that infection with H. pylori is associated with mucosal changes including chronic gastritis, mucosal atrophy, and intestinal metaplasia and dysplasia which are precursors to the development of intestinal type adenocarcinoma. Many studies have also linked regional diet with the risk of developing gastric carcinoma. These dietary links include high consumption of meat, smoked meats and salt-preserved foods. Worldwide, there has been a decline in the overall incidence of gastric cancer due to treatment of H. pylori and nutritional changes, including decreased salt intake, decreased use of salt-preserved foods, and the increase in diets of fruits and vegetables.
Gross features of gastric cancers are associated with characteristics of the two main categories, early gastric cancers and advanced gastric cancers. Tumors confined to the mucosa and submucosa, with or without nodal involvement are called early gastric cancers (EGC). There are three main types of endoscopic appearances of EGC: protruding (type I) superficial (type II) and excavating (type III). This classification scheme correlates with the incidence of metastatic disease to the nodes, seen rarely with type I, and more often with type III. Advanced carcinomas can be further subdivided using the Borrmann classification. This scheme categorizes advanced carcinomas that are polypoid (Type 1), ulcerated (Type 2), fungating (Type 3) and infiltrative (Type 4), the latter of which is also known as linitis plastica type.
Gastric cancers include a spectrum of histologic types and many microscopic classifications have been proposed. Most tumors exhibit variable histologic features, with predominance of one or more subtypes. The WHO recognizes specific types of gastric carcinoma (all are adenocarcinoma): papillary, tubular, mucinous, poorly cohesive (includes signet ring cell carcinoma). Rare histologic carcinoma variants comprise less than 5% of gastric carcinomas and include undifferentiated, hepatoid adenocarcinoma, gastric carcinoma with lymphoid stroma, squamous carcinoma, and adenosquamous carcinoma among others. The Laurén classification includes intestinal, diffuse, and indeterminate/unclassified types. Intestinal types form glands of variable differentiation, often arising in a background of intestinal metaplasia, whereas the diffuse types are composed of poorly cohesive cells with little to no gland formation that diffusely infiltrate the gastric wall. Mixed tumors in the Laurén classification contain roughly equal portions of intestinal and diffuse components. The intestinal type includes both papillary and tubular types from the WHO classifications, while the diffuse type includes signet ring cell and mucinous types. The indeterminate type includes the less common patterns such as adenosquamous and squamous cell types. The intestinal type of gastric adenocarcinoma is most common, while the diffuse type is more prevalent in younger patients and those with a genetic predisposition. Adenocarcinomas are graded as well differentiated (>95% glandular formation), moderately differentiated (50-95% glandular formation) and poorly differentiated (less than 50% glandular formation).
Although the vast majority of gastric carcinomas are sporadic (90%), certain hereditary links for gastric cancer have been identified. Hereditary diffuse gastric cancer syndrome is an autosomal dominant condition resulting from germline mutations in the gene (CDH1) encoding the cell adhesion protein E-cadherin. The gastric carcinomas in these patients arise in young individuals (teenage years and older) and histologically are signet ring cell (diffuse) carcinoma. Additional syndromes associated with an increased risk of developing gastric cancer include hereditary nonpolyposis colon cancer, Lynch, Li-Fraumeni, Peutz-Jeghers, and familial adenomatous polyposis syndromes.
The prognosis for patients with gastric cancer is directly related to tumor size, the depth of invasion, lymphovascular involvement and the presence of nodal disease. Mortality of gastric carcinoma has declined due to significant advances in the early detection of stomach cancer by endoscopy, with almost a quarter of all new cancers diagnosed as early cancers. EGC limited to the mucosa or mucosa and submucosa are often associated with a relatively good prognosis (approximately 90% 10-year survival). Advanced gastric carcinomas with invasion past the submucosa constitute the majority of gastric cancers and are associated with a significantly more aggressive course which worsens as the tumors extend through the muscularis propria and to the serosa.
Gastric carcinomas show variable patterns of spread, either by metastases, peritoneal dissemination, or direct extension. Intestinal type carcinomas that are well differentiated spread predominately through the vascular system, and often metastasize to the liver. In contrast, the diffuse carcinomas frequently spread to the peritoneal cavity. Those tumors with both intestinal and diffuse features are extremely aggressive, and frequently metastasize to both liver and the peritoneum. Thus, the pathologic determination of tumor type, tumor extent and nodal involvement is extremely important in determining prognosis and treatment. The treatment of gastric cancers ranges from endoscopic treatments, laparoscopy-assisted gastrectomy, and limited lymphadenectomies to total gastrectomy with extensive regional lymph node dissections. At least 15 lymph nodes are recommended for accurate staging. A multidisciplinary approach utilizing the endoscopic appearance, imaging findings, pathologic classification, etc. is necessary to determine the optimal surgical approach since complete surgical resection with appropriate lymph node dissection is correlated with the chance for long-term survival.
The differential diagnosis of mucinous adenocarcinoma of the stomach includes other histology types of primary tumors, such as invasive micropapillary carcinoma (IMPC) and papillary adenocarcinoma. Invasive micropapillary features in tumors were first noted in breast cancers. Similar histologic features have been also seen in other organs, including stomach, urinary tract, salivary gland, ovary, pancreas, colorectal and gallbladder. In the stomach, the recently described micropapillary subtype is rare, seen in less than 2% of stomach adenocarcinomas and is characterized by clusters of tumor cells lying within cleared spaces, mimicking lymphatic invasion. These cells typically show reverse polarity, with the nuclei orientated in the center of the clusters, and the apical surfaces orientated outward. IMPC may be seen in association with a tubular, papillary, mucinous or signet-ring cell type adenocarcinomas of the stomach and the amount of IMPC component varies, ranging from 10-90% of the tumor. However, there is no associated mucin unless this component co-exists with a typical mucinous carcinoma. The IMPC pattern has been shown to be an independent predictor of nodal metastases; up to 82% of patients have metastatic nodal disease at presentation, regardless of tumor size. Therefore, in patients with EGC it is important to report the IMPC pattern due to the more aggressive clinical course, since less aggressive surgical approaches (such as limited lymph node resections) are not optimal treatment options for this subtype.
Papillary gastric adenocarcinomas are typically exophytic, with malignant cells arranged along fibrovascular fronds. This type may also exhibit tubular and micropapillary morphology. Although this type of tumor is often well to moderately differentiated, it is often associated with lymph node and liver metastases.
Metastatic tumors to the stomach should be considered in the differential diagnosis of gastric carcinoma because of the important treatment and prognostic implications. And, the metastasis in the stomach can be the initial presentation of an undiagnosed cancer. These lesions are most frequently identified endoscopically and appear frequently as solitary (51-65%) or multiple (49-35%) lesions that mimic the gross and endoscopic appearances of primary gastric adenocarcinoma. Malignant melanoma has been reported to be the most frequent tumor to metastasize to the stomach comprising approximately a third of the reported cases, followed by metastatic lesions from lung, breast, and esophagus (squamous type). Carcinomas from these sites may share similar histological features, including micropapillary architecture. Thus, immunostains may be instrumental at confirming the origin of these tumors. SOX10, Melan-A and S-100 may help confirm a diagnosis of melanoma and exclude the possibility of carcinoma. GATA3 staining may be seen in tumors of both breast and bladder origin. Additional markers present in breast primaries may include estrogen receptor, mammaglobin, and gross cystic disease fluid protein 15. TTF1 and Napsin A positive immunostaining are useful in differentiating a possible metastatic lung carcinoma from breast, while TTF1 positivity would also be seen in most metastatic papillary thyroid carcinomas. Thus, a thyroglobulin stain may help with the latter differential.
Supplementary Questions
- Which of the following statements is true regarding the diagnosis of mucinous carcinoma of the stomach?
- Invasive micropapillary carcinoma is a subtype of gastric mucinous carcinoma.
- The diagnosis of gastric mucinous carcinoma is classified as intestinal type in the Laurén classification.
- The gastric mucinous carcinoma subtype represents approximately 10% of gastric cancers.
- The histologic categorization of gastric mucinous carcinomas requires > 90% extracellular mucin production.
- Which of the following statements is false regarding gastric carcinomas?
- H. pylori infection is the leading cause of distal gastric carcinoma.
- Hereditary diffuse gastric cancer syndrome is an autosomal dominant condition arising in older individuals (>50 years old).
- The development of gastric carcinoma has been linked to increased consumption of salt and salt preserved foods.
- The incidence of gastric cancer is decreasing worldwide.
- Which of the following statements is false regarding the clinical and pathologic characteristics of gastric carcinoma?
- Early gastric carcinomas are defined as tumors located within the mucosa and submucosa, with or without lymph node involvement.
- Patients with invasive micropapillary carcinoma often present with an advanced clinical stage.
- The prognosis for patients with gastric cancer is directly related to stage.
- Well-differentiated gastric carcinomas of intestinal type typically disseminate to the peritoneum.
References
- Eom DW, Kang GH, Han SH, et al. Gastric micropapillary carcinoma: a distinct subtype with a significantly worse prognosis in TMN stages I and II. Am J Surg Pathol. 2011;35:84-91.
- Hamilton SR, Aaltonen LA, (eds). Fenoglio-Preiser C, Carneiro F, Correa P, et al. Tumours of the stomach. In: Hamilton SR, Aaltonen LA, eds. Tumours of the stomach. World Health Organization Classification of Tumours: Pathology and Genetics of Tumours of the Digestive System. Lyon, FR: IARC Press;2000:37-52.
- Green LK. Hematogenous metastases to the stomach. A review of 67 cases. Cancer. 1990;65(7):1596-1600.
- Lauwers G. Epithelial neoplasms of the stomach. In: Odze RD, Goldblum JR, Crawford JM, eds. Surgical Pathology of the GI Tract, Liver, Biliary Tract, and Pancreas. 2nd Ed. Philadelphia, PA: Saunders; 2009:563-579.
- Lauwers GY, Carneiro F, Graham DY, et al. Gastric carcinoma. In: Bosman FT, Carneiro F, Hruban RH, Theise ND, eds. WHO Classification of Tumours of the Digestive System. 4th ed. Lyon, FR: IARC Press; 2010:48.
- Hamilton SR, and Aaltonen LA (eds). Niederau C, and Sobin LH. Secondary tumors of the stomach. Hamilton SR, Aaltonen LA, eds. World Health Organization Classification of Tumour: Pathology and Genetics of Tumours of the Digestive System. Lyon, FR: IARC Press; 2000:66-67.
- Oda, Kondo H, Yamao T, et al. Metastatic tumors to the stomach: Analysis of 54 patients diagnosed at endoscopy and 347 autopsy cases. Endoscopy. 2001;33(6):507-510.
- Ushiku T, Matsusaka K, Iwasaki Y, et al. Gastric carcinoma with invasive micropapillary pattern and its association with lymph node metastasis. Histopathology. 2011;59:1081-1089.
Author
2016
Tamera J. Lillemoe, MD
Surgical Pathology Committee
Hospital Pathology Associates and Allina Health Laboratory
Minneapolis, MN
Answer Key
- The gastric mucinous carcinoma subtype represents approximately 10% of gastric cancers. (b)
- Hereditary diffuse gastric cancer syndrome is an autosomal dominant condition arising in older individuals (>50 years old). (b)
- Well-differentiated gastric carcinomas of intestinal type typically disseminate to the peritoneum. (d)