- Home
- Member Resources
- Pathology Case Challenge
- Soft tissue
Clinical Summary
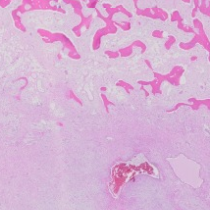
A 13-year-old boy presents with a soft tissue mass in the posterior aspect of the right knee. On palpation the mass is round and hard measuring 5.0 cm in diameter. Imaging studies include an ultrasound demonstrating a hyperechoic shell with a hypoechoic center. Gross examination shows a round mass with a calcific outer rim and an edematous fibrous appearing core.
Master List:
- Extraskeletal osteosarcoma
- Fibrodysplasia ossificans progressiva
- Myositis ossificans circumscripta
- Parosteal osteosarcoma
- Periosteal osteosarcoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2015, case 21 and is a myositis ossificans circumscripta.
Criteria for Diagnosis and Comments
Myositis ossificans circumscripta (MO) is an ossified soft tissue mass seen in patients with antecedent trauma or other tissue injury. It typically occurs intramuscularly but may present in adipose tissue or associated with periosteum. The lesion initially presents as a zonated soft tissue mass with a hyperemic periphery and a hypocellular center. Within a few weeks the periphery undergoes an osseous metaplasia resulting in so-called eggshell ossification. Peripheral to the calcified shell there is usually an edematous fibrous layer. The characteristic rim of bone with a non-calcified center can be observed with multiple imaging techniques, however ultrasound appears to highlight the zonation of the lesion earlier than other techniques. Histologically, the most obvious finding is the ossified layer with central fibrosis. The lesion lacks significant inflammation despite its association with tissue injury. The bone displays a monomorphous osteoblastic rimming without atypia. The fibrous stroma resembles nodular fasciitis, cellular but lacking true atypia. Because of the cellularity and proliferative activity early lesions can sometimes be over interpreted as sarcoma. Over time the ossified shell thickens but a fibrous core generally remains, and becomes more collagenized and less cellular. Lesions may persist or can occasionally be resorbed. MO is benign and requires removal only if there is a mechanical or cosmetic disruptive mass effect. The current case is a fairly mature lesion with a thick osseous rim.
The pathogenesis of the MO is poorly understood but some cases have been shown to have rearrangements in the USP6 gene suggesting an association with aneurysmal bone cyst.
Fibrodysplasia ossificans progressiva (myositis ossificans progressiva) is a progressive heterotopic ossification that is caused by an autosomal dominant mutation in a gene that encodes a cell surface receptor (Activin A receptor type I). This receptor binds bone morphogenetic proteins. The mutation results in a constitutively activated receptor resulting in bone formation. In addition to the progressive bone formation patients suffer from malformed digits, especially the great toe. Patients present, usually in early childhood, with intramuscular, edematous soft tissue nodules that ossify. Soft tissue injury is frequently associated with new lesions. Ossification is intermittent but progressive and generally progresses from axial to appendicular muscles resulting in severe compromise of muscle function. By the third decade of life, most patients are confined to a wheelchair and with a secondary “cage” of calcification have difficulty with respiration. The lesions of this rare disorder have frequently been initially misdiagnosed as sarcomas. Early lesions resemble nodular faciitis with fibroblasts in an edematous background and modest lymphocytic inflammation. Over time the stroma collagenizes and central ossification ensues. Nodules of calcification can coalesce, eventually replacing muscle bellies.
Extraskeletal osteosarcoma is the most important differential diagnosis since it is a bone-forming soft tissue tumor with a very different prognosis from MO. Extraskeletal osteosarcoma faithfully recapitulates bone osteosarcoma and can display all of the variants. The most common pattern, as in bone, is the osteoblastic pattern. Atypical spindle cells are associated with tumor osteoid. The osteoid can display several patterns including trabecular, lacy or sheet like. Mitoses, including atypical mitoses are common. In contradistinction to MO, ossification typically occurs in the center of the lesion. Overall the degree of atypia should prevent confusion between the two lesions. Like bone, other variants include chondroblastic, telangiectatic, and small cell osteosarcoma. Extraskeletal osteosarcoma is a highly malignant tumor with a poor prognosis.
Parosteal and periosteal osteosarcoma are tumors that arise from the surface of bones. Because MO can be associated with periosteum, there is some possibility of confusion. Parosteal osteosarcoma is composed of well-formed bone trabeculae with a bland, hypocellular, spindle cell proliferation that is in the marrow space. Some areas may have minimal bone formation. Because the lesion is bland and may have areas with little bone formation, MO may be in the differential diagnosis however true zonal architecture is lacking and MO should have more orderly bone maturation. Parosteal osteosarcoma has more centrally located bone formation with less away from bone and a cartilage cap, whereas MO has peripheral bone formation, with maturation at the periphery. Periosteal osteosarcoma, an intermediate grade surface chondroblastic osteosarcoma, is a pleomorphic sarcoma producing osteoid and cartilage. Its main distinction from classical osteosarcoma is its location and the distinction from MO should not usually be problematic.
Supplementary Questions
- Which of the following is true regarding myositis ossificans (circumscripta)?
- Atypical osteoblasts are common
- Early lesions demonstrate a zonal pattern on imaging.
- Malignant transformation commonly occurs.
- Ossification typically occurs at the center of the lesion.
- Ossification is progressive a zonal patter on imaging.
- Which of the following is caused by a mutation in the gene that encodes Activin A receptor?
- Extrasketal osteosaecoma
- Fibrodysplasia ossification progressiva
- Myositis ossificans
- Parosteal osteosarcoma
- Periosteal osteosarcoma
- Extraskeletal osteosarcoma is distinguished from myositis ossificans primarily by the presence of significant cytologic atypia.
- True
- False
References
- Ackerman LV. Extra-osseous localized non-neoplastic bone and cartilage formation (so-called myositis ossificans): clinical and pathological confusion with malignant neoplasms. J Bone Joint Surg Am. 1958;40-A(2):279-298.
- Fanburg-Smith JC, Bratthauer GL, Miettinen M. Osteocalcin and osteonectin immunoreactivity in extraskeletal osteosarcoma: a study of 28 cases. Hum Pathol. 1999;30(1):32-38.
- Lacout A, Jarraya M, Marcy PY, Thariat J, Carlier RY. Myositis ossificans imaging: keys to successful diagnosis. Indian J Radiol Imaging. 2012;22(1):35-39.
- Pignolo RJ, Shore EM, Kaplan FS. Fibrodysplasia ossificans progressiva: diagnosis, management, and therapeutic horizons. Pediatr Endocrinol Rev. 2013;10:437-448.
- Rosai J, Ackerman LV. Rosai and Ackerman's Surgical Pathology. 10th ed. New York, NY: Mosby;2011.
Authors
Jason Brazelton, MD
Pathology Resident
University of Alabama at Birmingham
Birmingham, AL
Thomas Winokur, MD
Surgical Pathology Committee
Department of Pathology
University of Alabama at Birmingham
Birmingham, AL
Answer Key
- Early lesions demonstrate a zonal pattern on imaging. (b)
- Fibrodysplasia ossificans progressiva (b)
- True (a)