- Home
- Member Resources
- Pathology Case Challenge
- Skin and soft tissue of right forearm
Clinical Summary
A 45-year-old healthy construction worker sustains a superficial laceration to his arm at his worksite. He does not receive any immediate medical attention for the cut. Several weeks later he develops generalized erythema and discoloration of the skin of the upper extremity in the region of previous trauma. He finally requests medical attention due to pain and stiffness that prevents him from working. He requires an extensive surgical debridement of the skin and subcutaneous tissue for control of disease. At the time of surgery, material from the soft tissue wound is submitted for culture.
Master List:
- Atypical mycobacterial infection
- Cat scratch disease (Bartonella henselae)
- Fungal infection due to hyalohyphomycotic organism (Scedosporium Apiospermum)
- Granuloma annulare
- Necrobiosis lipoidica
- Rheumatoid nodule
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2015, case 22 and is a fungal infection due to hyalohyphomycotic organism (Scedosporium Apiospermum).
Criteria for Diagnosis and Comments
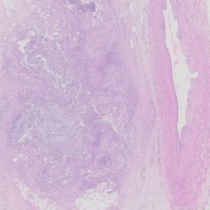
Histologic sections reveal numerous granulomas in the superficial and deep dermis of variable size and shape. In some sections, the granulomatous inflammation becomes confluent, simulating a geographic type of necrosis. The centers of the granulomas contain necrotic debris, rare neutrophils and, in some sections, partially calcified fungal hyphae. The granulomas are surrounded by histiocytes, both single and multinucleate forms. Often these form a pseudo-palisading type of arrangement. Gomori silver staining reveals slender septate fungal hyphae with acute angle branching. Culture of the lesion grew Scedosporium Apiospermum.
Scedosporium belongs to a class of fungal organisms known as hyalohyphomycoses. Hyalohyphomycotic organisms are characterized in tissue sections as hyaline hyphae (without pigment in the wall) as opposed to the phaeohyphomycses, which are pigmented. The hyalohyphomyocotic group is very diverse and includes a number of organisms including Fusarium spp., Aspergillus spp., Scedosporium spp. and others. Scedosporium is considered an emerging fungal pathogen; incidence of opportunistic infection with this organism is increasing, particularly in the immunocompromised patient population. Scedosporium ssp. can be isolated from a variety of environmental sources including rural soils, polluted waters, composts and the manure of cattle and fowl.
In immunocompetent individuals, infection by Scedosporium spp. will most often occur from direct inoculation of fungi into the skin or soft tissue after local, penetrating trauma. Rarely, infections will be acquired from inhalation of fungal spores or ingestion of contaminated food or water. In addition, there are a few reported cases of Scedosporium infection in near drowning victims. The clinical spectrum of infection in healthy individuals includes otitis, sinusitis, skin, soft tissue, and bone and joint infections. Disseminated infections occur chiefly in the immunocompromised patient population including transplantation patients and individuals with acquired immunodeficiency syndrome (AIDS). In severely immunocompromised patients, skin infections can be rapidly fatal. Immunocompromised patients are also at risk for pneumonia, meningitis, and brain infections. Identification of Scedosporiasis is important as this organism is usually widely resistant to treatment with Amphotericin B.
The histological differential diagnosis of Scedosporium infection is broad and includes a number of conditions which produce necrotizing, granulomatous inflammation of the superficial soft tissues. Firstly, Scedosporium infection needs to be distinguished from the other hyalohyphomycotic organisms, particularly the opportunist Aspergillus ssp and Fusarium spp. This usually cannot be done by morphology alone and will require either culture or a molecular method of species confirmation. Other pathogens to be considered in the differential diagnosis would include Mycobacterium tuberculosis, atypical mycobacteria or Bartonella henselae, the causative agent of cat scratch disease. In addition there are a number of necrobiotic granulomatous processes not associated with a specific infectious agent. The latter would include granuloma annulare, necrobiosis lipoidica, and rheumatoid nodule.
Mycobacterium tuberculosis infection of the skin is relatively rare. Skin lesions are usually a late complication of disseminated tuberculosis. Atypical mycobacterial infections of the skin and superficial soft tissues are more common and are often due to either Mycobacterium ulcerans or Mycobacterium marinum. Infection with Mycobacterium ulcerans is also known as Buruli ulcer and has been reported in areas of Central and West Africa as well as Southeast Asia and Mexico. Mycobacterium ulcerans produces extensive coagulative necrosis involving the dermis and subcutaneous fat. A granulomatous response occurs in long standing, chronic infections. Mycobacterium marinum is an organism that thrives in brackish water, swimming pools, and fish tanks. Cutaneous lesions often erupt after superficial trauma and exposure to contaminated water. In atypical mycobacterial infections the specific type of mycobacteria can be difficult to identify in histologic sections and either culture or molecular (polymerase chain reaction (PCR) based) confirmation is needed for definitive identification of the organism.
Cat scratch disease produces suppurative or granulomatous reactions, but these histologic changes are largely confined to lymph nodes adjacent to the site of inoculation. The clinical course of cat scratch disease is characterized by the appearance of a primary skin lesion: a macule, papule, or vesicle, within three to five days after a bite or scratch from a cat. Lymphadenopathy occurs about one to three weeks later and is often accompanied by systemic symptoms including fever and malaise. Cat scratch disease is attributed to infection from the gram negative bacteria Bartonella henselae or occasionally Bartonella quintana. The organism can be identified in histologic sections with a Warthin-Starry stain but PCR is a more sensitive method of confirmation. In immunocompetent patients, no treatment is necessary as the disease will most often resolve spontaneously. Immunocompromised patients with Bartonella infection are at risk for development of bacillary angiomatosis.
Granuloma annulare (GA) is a relatively common, chronic skin condition of unknown etiology, characterized by necrobiotic granulomas. The condition affects both children and adults and women are four times more likely to be afflicted than men. Clinically GA often appears as small raised bumps that form an annular or ring-like configuration, often with a central area of depression. GA can be subdivided into different categories based on the clinical presentation, location, and severity of the lesions. Localized GA is the most common subtype and tends to occur on the distal extremities of children and young adults. The diffuse or generalized subtype of GA is less common, accounting for about 15% of all cases. Diffuse GA tends to affect adult patients and appears in more proximal locations including the proximal extremities and the trunk. The deep subtype of GA tends to occur on the scalp, fingers or shins, and clinically resembles a rheumatoid nodule. The perforating form is typically limited to the dorsum of the hands and fingers in children. Most instances of localized GA involve a solitary lesion which will regress spontaneously. The generalized or diffuse form of GA often has a more protracted course and responds poorly to therapy.
Histologically, GA appears as one or more areas of necrobiosis in the superficial or deep dermis. The necrobiotic foci are surrounded by a peripheral rim of histiocytes which often align in a palisading type of pattern. Occasionally, the centers of the necrotic foci can have neutrophils or nuclear fragments. There is often a rim of chronic inflammation, and rare multinucleate giant cells may be present. A perivascular infiltrate containing lymphocytes and histiocytes is usually present and eosinophils are identifiable in about half of cases. The central necrobiotic foci contain increased amounts of connective tissue mucins which can appear as basophilic stringy material between collagen bundles. Staining for colloidal iron or alcian blue is often helpful in demonstrating this feature.
Necrobiosis lipoidica (NL) is classically associated with diabetes but skin lesions will frequently present prior to the onset of impaired glucose tolerance or diabetes. NL tends to develop on the anterior lower extremity (shin) and is often bilateral. The average age of onset of NL is 35 years; but children are infrequently affected. Women are more frequently afflicted than men (3:1). Adults and children with insulin-dependent diabetes and NL are at high risk for diabetic nephropathy and retinopathy. Clinically NL appears as raised papules which enlarge radially to become patches or plaques with an atrophic or depressed center. Some lesions will show spontaneous regression, but many are persistent and chronic. Minor trauma will often cause ulceration of the involved skin surface. Interestingly, the presence and severity of NL skin lesions does not correlate with control of serum glucose levels.
Histologically, NL appears as poorly delineated areas of necrosis, often layered between areas of inflammation, imparting a stacked "lasagna-like" or “layer-cake” appearance to the lesion. NL tends to involve the full thickness of the dermis and often extends into the subcutaneous adipose tissue. Large foci of necrosis coalesce to form necrobiotic granulomas surrounded by histiocytes. There is often an associated septal panniculitis. Necrotizing vasculitis and necrosis of skin adnexal structures are sometimes seen adjacent to areas of necrobiosis.
Rheumatoid nodules (RNs) are another form of necrobiotic granuloma that occur in individuals with rheumatoid arthritis (RA). Formation of RNs can also occasionally be seen in association with other forms of autoimmune disease including: systemic lupus erythematosus, scleroderma, and ankylosing spondylitis. The development of RNs is an inconsistent feature of RA, occurring in about 20 to 25% of afflicted patients at some point in the course of their disease. RNs tend to develop in individuals with severe arthritis and a high titer of rheumatoid factor. RNs tend to occur in sites associated with a bony prominence such as the elbow or the finger joints. Rarely RNs will occur in deep seated organs, particularly the heart, lung, and pleura.
RN appears, histologically, as one or more areas of necrobiosis surrounded by a well developed palisade of histiocytes. The nodules may also contain occasional lymphocytes, neutrophils, mast cells, and multinucleate giant cells. The central necrobiotic focus is most often eosinophilic and homogenous in appearance. Old nodules may become fibrotic and cystic with large clefts within the necrobiotic foci. The centers of the lesions contain fibrin as opposed to mucin, a feature which can be used to distinguish RN from the deep variant of granuloma annulare.
Supplementary Questions
- Which of the following is the most likely source of Scedosporium infection in an immunocompetent host?
- Consumption of contaminated shellfish
- Contact with another infected individual
- Direct inoculation from a penetrating type of trauma.
- Exposure of abraded skin to fish tank water.
- Travel to an endemic area (West Africa)
- Which of the following statements best describes necrobiosis lipoidica?
- It is always seen in association with diabetes.
- It is usually confined to the upper extremity.
- It is histologically characterized by layers of necrosis and inflammation.
- Men are more likely to be affected than women.
- The severity of the skin lesions correlates with control of serum glucose levels.
- Which of the following statements best describes rheumatoid nodule?
- Histologically, rheumatoid nodule can be difficult to distinguish from the deep variant of granuloma annulare.
- Rheumatoid nodule is often the first and only manifestation of rheumatoid arthritis.
- Rheumatoid nodule is seen only in association with rheumatoid arthritis.
- The location of rheumatoid nodule is limited to the extremities.
- The necrobiotic center contains Alcian blue positive mucin.
References
- Koneman EW, Allen SD, Janda WM, Schreckenberger PC, Winn WC. Color Atlas and textbook of diagnostic Microbiology. 5th ed. Philadelphia, PA: Lippincott; 1997:918-925.
- Liao CH, Lai CC, Ding LW, et al. Skin and soft tissue infection caused by non-tuberculous mycobacteria. Int J Tuberc Lung Dis. 2007:11:96-102.
- Lynch JM, Barrett TL. Collagenolytic (necrobiotic) granulomas: part I-- the “blue” granulomas. J Cutan Pathol. 2004;31:353-361.
- Lynch JM, Barrett TL. Collagenolytic (necrobiotic) granulomas: part II—the “red” granulomas. J Cutan Pathol. 2004;31:409-418.
- Mujeeb I, Sutton DA, Fothergill AW, Rinaldi MG, Pfaller MA “Fungi and Fungal Infections” in McClatchey KD (ed). Clinical Laboratory Medicine. 2nd ed. Philadelphia, PA: Lippincott; 2002:1125-1156.
- Weedon A. Skin Pathology, 2nd ed. London, UK: Churchill Livingstone; 2002:193-220.
Author
Leslie G Dodd, MD
Surgical Pathology Committee
University of North Carolina
Chapel Hill, NC
Answer Key
- Direct inoculation from a penetrating type of trauma (c)
- It is histologically characterized by layers of necrosis and inflammation. (c)
- Histologically, rheumatoid nodule can be difficult to distinguish from the deep variant of granuloma annulare. (a)