- Home
- Member Resources
- Pathology Case Challenge
- Right Ovary
Clinical Summary
A 60-year-old woman presents with abdominal pain. Physical examination reveals a large abdominal mass. A CT scan of the abdomen and pelvis shows a large cystic right ovarian mass extending from the pelvis to the abdominal cavity. She undergoes total abdominal hysterectomy with bilateral salpingo-oophorectomy, and bilateral pelvic and para-aortic lymph node dissections. Gross examination shows a markedly dilated unilocular ovarian cystic mass that measures 10.0 cm in greatest dimension, filled with thick brown, slightly mucinous fluid. The cyst contains a solid 6.0 x 3.5 cm area; scattered, variably thickened, coarsely nodular and broad-based papillary excrescences line the interior wall.
Master List
- Clear cell carcinoma
- Dysgerminoma
- Krukenberg tumor
- Metastatic renal cell carcinoma
- Serous borderline tumor
- Yolk sac tumor
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2014, case 19 and is a clear cell carcinoma.
Criteria for Diagnosis and Comments
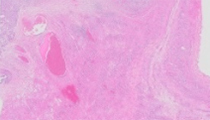
Sections show fragments of an ovarian cyst wall lined by malignant epithelial cells with abundant clear to slightly eosinophilic foamy cytoplasm, medium-large sized round-oval nuclei, and large prominent eosinophilic nucleoli. Focally the cells are arranged in tubulocystic patterns with prominent hobnail cells. In other areas, the cells are arranged in short and round papillae with hyalinized cores without hierarchical branching. These histologic features are characteristic of clear cell carcinoma (CCC) of the ovary.
CCC is the second most common type of ovarian epithelial cancer, accounting for 5–25% of all surface epithelial ovarian carcinomas. These neoplasms typically occur in the fifth to sixth decades and are more prevalent in Asian populations. Two-thirds of women with ovarian CCC are nulliparous. The clinical presentation is usually that of pelvic/abdominal pain or abdominal swelling related to an enlarging abdominal mass. Many (50–70%) have associated pelvic endometriosis and/or endometriosis involving the ovary (25%). Most cases (80%) are unilateral, and approximately 40–60% of patients present with stage I disease. No histologic features have been definitively identified that can predict prognosis. Patients with CCC have an increased rate of developing thromboembolic complications—up to 40% of patients, which is double that of patients with other types of surface epithelial carcinomas.
Although recent literature suggests that patients with stage I disease may be cured by surgery alone, most CCCs are treated with optimal debulking and adjuvant chemotherapy. Patients with stage IC/II and higher stage disease have poorer survival rates than those with surface epithelial carcinomas of other cell types. These tumors generally show a poor response rate to chemotherapy, and chemoresistance to platinum-based therapy is common. Radiation therapy has been recently shown to be effective in improving overall survival in some patients.
Grossly, CCCs are usually solid or cystic (unilocular or multilocular), with variable amounts of necrosis and hemorrhage. These neoplasms may measure up to 30.0 cm (mean, 15.0 cm), and are frequently associated with endometriosis.
Microscopically, CCC is characterized by polyhedral high grade cells with abundant clear and/or eosinophilic granular cytoplasm and hobnail cells with scant cytoplasm and enlarged bulbous nuclei that protrude into the lumens of the cystic spaces. Cells can also be cuboidal or flat. The cytoplasm is glycogen rich and PAS positive. These carcinomas often show an admixture of tubulocystic, papillary, and solid patterns. The complex papillae with dense hyaline basement membrane material in the cores of the papillae are hallmarks of this tumor. Approximately 25% of cases will also have associated hyaline bodies. Mixed clear cell and other histologic type carcinomas are very rare. Most historic cases that were diagnosed as mixed clear cell and endometrioid or serous carcinoma have been shown to be either pure endometrioid carcinomas with clear cells or high grade serous carcinomas with clear cells. Benign and borderline clear cell tumors are very rare and almost always have an adenofibromatous component.
Molecular studies have revealed that 50% of CCC cases have tumor suppressorARID1A mutations, a finding also seen in endometrioid carcinomas and in adjacent endometriosis. Hepatocyte nuclear factor 1 (HNF1), a transcription factor, has been shown to be upregulated in CCC as well as in atypical endometriosis, and may be a potential therapeutic target. Thus, atypical endometriosis has emerged as a probable precursor lesion. Up to 40% of CCC cases have PIK3CA mutations but BRCA1/2 mutations are only rarely present. Additionally, CCC has been identified to be associated with Lynch syndrome.
CCCs generally express a CK7 and EMA positive and CK20 negative profile. They may also express B72.3, CD15 (Leu-M1), CEA, CA125 (in approximately 50% of cases) and rarely, AFP. CCCs are typically ER negative (to minimally positive) and WT-1 negative, in contrast to most other surface ovarian carcinomas. HNF1 has also been shown to be a specific marker for CCC and can help distinguish CCC from serous and endometrioid carcinomas.
CCCs with a predominantly diffuse pattern may be confused with a dysgerminoma. However, dysgerminomas typically occur in second and third decades, and the young age of patients provides strong evidence against the diagnosis of CCC. Furthermore, CCC show an admixture of other architectural patterns such as papillary and tubulocystic, whereas dysgerminomas typically exhibit a diffuse, solid architecture. The inflammatory infiltrate is predominantly lymphocytic in dysgerminoma while CCC contains mainly plasma cells. Immunohistochemistry is useful in this differential; cytokeratin and EMA are strongly and diffusely positive in CCC, but weakly positive or negative in dysgerminoma. And, OCT3/4 is positive in dysgerminoma but negative in CCC.
Serous borderline tumors may contain occasional clear and/or hobnail cells but generally do not exhibit the characteristic hyalinized cores seen in CCC. High grade serous carcinomas, in contrast to CCC, typically present at a higher stage, and frequently are associated with tubal intraepithelial carcinoma. Serous tumors have a higher association withBRCA mutations, have a very low frequency of PIK3CA mutations, and show no mutations of ARID1A (in contrast to CCC).
CCC may share histologic similarities with yolk sac tumor and may also occur in younger women, although CCC is rare under 40 years of age. Yolk sac tumor is associated with a reticular growth of primitive tumor cells within a loose background stroma, papillary Schiller-Duval bodies and elevated serum levels of AFP. Immunohistochemical staining for AFP is less helpful, since it can also be seen in up to 30% of CCC. Thus, CK7 and EMA positivity may be more useful in confirming a diagnosis of CCC.
Metastatic carcinomas may show histologic similarities with CCC, including renal cell carcinomas and Krukenberg tumors. Features favoring a diagnosis of metastatic carcinoma include a known extraovarian primary tumor, bilaterality, and lack of the typical admixture of hyaline papillary patterns of CCC.
Supplementary Questions:
- Which of the following statements is correct regarding clear cell carcinoma of the ovary?
- Clear cell carcinoma has a better prognosis compared to other surface epithelial carcinomas.
- Clear cell carcinomas are associated with pelvic endometriosis and nulliparity.
- Clear cell carcinomas are typically sensitive to platinum-based therapy.
- Most cases of stage I clear cell carcinoma are effectively treated with chemotherapy.
- Most clear cell carcinomas present as stage III-IV disease.
- Which immunohistochemical profile is most consistent with clear cell carcinoma?
- CK-, EMA-, OCT4+, CD117+, PLAP+, CD15-
- CK7-, AE1/AE3+, EMA-, AFP+, HNF1+
- CK7-, CK20-, CA125-, CD10+, CEA+, CD15+
- CK7+, CK20-, CA125+, ER-, WT-1-, HNF1+
- CK7+, CK20-, CA125+, ER+, WT-1+, HNF1-
- Which gross description is most consistent with the appearance of clear cell carcinoma?
- Bilateral, solid, with a white or yellow cut surface
- Large cystic mass with soft papillary projections and surface papillary excrescences
- Solid mass with homogenous lobulated rubbery-white to tan cut surface
- Solid, fleshy, grey to tan mass, with focal honeycomb (microcystic) appearance
- Thick walled unilocular cystic mass with fleshy nodules
References
- Montag AG, Jenison EL, Griffiths CT, et al. Ovarian clear cell carcinoma: a clinicopathologic analysis of 44 cases. Int J Gynecol Pathol. 1989;8:85-96.
- Nucci MR, Olivia E, Gynecologic Pathology: A Volume in Foundations in Diagnostic Pathology Series. Philadelphia, PA: Elsevier Churchill Livingstone; 2009:432-436.
- Vang R, Whitaker BP, Farhood AI, et al. Immunohistochemical analysis of clear cell carcinoma of the gynecologic tract. Int J Gynecol Pathol. 2001;20:252-259.
- Anglesio MF, Carey MS, Kobel M, MacKay H, Huntsman DG, et al. Clear cell carcinoma of the ovary: a report from the first ovarian clear cell symposium, June 24th,2010. Gynec Oncol. 2011;121:407-415.
- Prat J. Ovarian carcinomas: five distinct diseases with different origins, genetic alterations, and clinicopathological features. Virchows Arch. 2012;460:237-249.
- del Carmen MG, Birrer M, Schorge JO. Clear cell carcinoma of the ovary: a review of the literature. Gynecol Oncol. 2012;126:481-490.
- Higashiguchi A et al: Specific expression of hepatocyte nuclear factor-1beta in the ovarian clear cell adenocarcinoma and its application to cytological diagnosis. Cancer Sci. 2007;98(3):387-391.
- Offman SL, Longacre TA. Clear cell carcinoma of the female genital tract (not everything is as clear as it seems). Adv Anat Pathol. 2012;19:296-312.
Authors
2014
Tetyana Mettler, MD
Pathology Resident
University of Minnesota
Minneapolis, MN
Tamera J. Lillemoe, MD FCAP
Surgical Pathology Committee
Hospital Pathology Associates
Abbott Northwestern Hospital
Minneapolis, MN
Answer Key
- Clear cell carcinomas are associated with pelvic endometriosis and nulliparity (b).
- CK7+, CK20-, CA125+, ER-, WT-1-, HNF1+ (d).
- Thick walled unilocular cystic mass with fleshy nodules (e).