- Home
- Member Resources
- Pathology Case Challenge
- Parotid Gland
Clinical Summary
A 79-year-old woman initially presents with facial twitching and is otherwise asymptomatic. Imaging studies performed to rule out the possibility of a stroke reveal a 2.4 cm right parotid gland mass with central calcification and enlarged level II and III lymph nodes. The patient presents again 8 months later with interval increase of her right parotid mass, which now involves the entire parotid gland and measures 7 cm. Additionally, the overlying skin is thickened suggestive of cutaneous involvement, and one of the right level II lymph nodes is now enlarged to 2.0 cm. The resection specimen includes the right parotid gland, levels Ib through IV neck dissection, and a partial auriculectomy. The earlobe, submandibular gland, and jugular vein are unremarkable. The 7.2 × 5.5 × 3.2 cm parotid mass shows gross extension to skin and to the cartilaginous portion of the external auditory canal.
Master List
- Adenoid cystic carcinoma with high-grade transformation
- Epithelial-myoepithelial carcinoma with high-grade transformation
- Metastatic mammary carcinoma
- Salivary duct carcinoma
- Squamous cell carcinoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2015, case 01, and is salivary duct carcinoma.
Criteria for Diagnosis and Comments
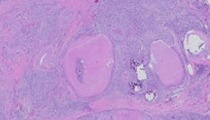
The histological sections reveal a highly infiltrative epithelioid neoplasm with extensive perineural and angiolymphatic invasion. Most of the sections show the neoplastic proliferation involving skin, subcutaneous tissue, and skeletal muscle. Extraparotid extension is recognized grossly, a fact that is important in assigning pathologic stage. The overlying skin is ulcerated, precluding evaluation for any potential cutaneous squamous cell carcinoma in situ component. Some tissue sections show residual atrophic parotid tissue and cartilage of the external auditory canal. Gross recognition of earlobe and external auditory canal helps to distinguish these foci of cartilaginous tissue from possible residual pleomorphic adenoma. The neoplastic proliferation extensively involves regional lymph nodes, entirely replacing some of them, and extends to soft tissue margins of resection. The solid growth is accompanied by linear arrays of single cell infiltration, micropapillary and cribriform growth patterns. Comedo-type necrosis and microcalcifications are identifiable in some tissue sections. There is no evidence of pre-existing pleomorphic adenoma. Cytologically, the neoplastic cells are characterized by eosinophilic cytoplasm, pleomorphic nuclei, and prominent nucleoli. On routine H&E stained sections, only ductal type neoplastic cells are seen. The presence of "snouts" at luminal aspects of some ductal cells is indicative of apocrine-type secretion. Intraductal mucin secretion is minimal and intracytoplasmic mucin droplets are rare. Despite the overall eosinophilic appearance, there is no evidence of keratinization or desmosomes.
Immunohistochemically, neoplastic cells are positive for cytokeratin 7, gross cystic disease fluid protein - 15, mammaglobin, and androgen receptor (AR). The neoplasm is negative for S-100 protein, estrogen receptor, progesterone receptor, and p63. Overall, these are features of salivary duct carcinoma (SDC).
The differential diagnosis includes neoplasms of salivary and non-salivary origins, such as squamous cell carcinoma, metastatic adenocarcinoma of breast origin (and prostate origin in male patients).
Squamous cell carcinoma is one of the most common mimickers of SDC. Cutaneous squamous cell carcinoma may involve the parotid gland by direct extension or due to extensive extranodal spread after initial metastasis to intraparotid lymph nodes. Immunohistochemical studies are helpful in distinguishing clear cell and acantholytic variants of cutaneous squamous cell carcinomas and non-keratinizing mucosal squamous cell carcinomas from SDC. In brief, almost all squamous cell carcinomas are p63 positive, while SDC, like most adenocarcinomas, are p63 negative.
In our case, the lack of pre-existing pleomorphic adenoma highlights the need to consider the possibility of metastases from occult adenocarcinoma of breast origin. The immunoprofile of neoplastic cells, involvement of regional lymph nodes, and the knowledge of imaging studies initially localizing carcinoma to the parotid gland argue against the possibility of metastatic breast carcinoma. Also, while p63 is negative in the neoplastic cells, it focally highlights a linear residual basal cell layer, confirming an intra-ductal SDC component. It is unclear whether such intra-ductal SDC represents an in situ component or duct cancerization. In a male patient, metastatic prostate adenocarcinoma has to be considered in the differential diagnosis of a tumor that is AR positive and p63 negative. Of note, fewer than 5% of SDC express prostate specific antigen or prostatic acid phosphatase.
For most salivary-type carcinomas, the histologic classification defines the grade. For instance, all SDC are of high grade and the differential diagnosis for SDC can be focused on salivary-type carcinomas with high-grade transformation. Since about 90% of SDC are AR-positive, the diagnostic decision is made easier and more objective with just two immunohistochemical stains - AR and p63. Before accepting the diagnosis of AR-negative SDC, the possibility of other types of salivary carcinoma with high-grade transformation has to be addressed. Areas of high-grade transformation in adenoid cystic carcinoma and epithelial-myoepithelial carcinoma are characterized by necrosis and closely mimic SDC. Adenoid cystic carcinoma and epithelial-myoepithelial carcinomas with high-grade transformation usually retain some well-differentiated areas composed of a biphasic cellular population (i.e., inner ductal cells and outer basal/myoepithelial cells). In such areas, the outer basal/myoepithelial cells will be highlighted by p63.
TNM staging of salivary tumors is not influenced by histologic type, but depends on anatomic site of origin. For instance, tumors arising from minor salivary glands should be staged similarly to other non-salivary carcinoma types affecting paranasal sinuses or oral cavity. Only salivary carcinomas arising in major salivary glands are classified according to a distinct set of rules. Most SDC arise in the parotid gland and extraparenchymal (extraparotid) extension affects pT classification independently of tumor size. Clinical or gross evidence of extraparotid soft tissue invasion is needed to document the presence of extraparenchymal invasion and indicates a pT3, at least. In other words, microscopic finding of extension into a skeletal type muscle is insufficient to document extraparenchymal tumor extension. Invasion of the facial nerve, skin (as in our case), mandibular bone, or encasement of the carotid artery is indicative of pT4.
Current management of SDC relies on surgical resection followed by radiation and traditional systemic chemotherapeutic agents for metastatic disease. Newer treatment modalities include androgen deprivation or targeting of human epidermal growth factor receptor-2 (HER2) which is frequently overexpressed. HER2 fluorescence in situ hybridization studies in our case showed no amplification.
Genetic alterations that may lead to activation of the phosphoinositide 3-kinase (PI3K) pathway have been found in 20-50% of SDC. PI3K pathway activation may be due to mutations in the gene encoding the p110α catalytic subunit of PI3K (PIK3CA) or secondary to phosphatase and tensin homolog (PTEN) deletion. In our case, a PIK3CA exon 20 p.H1047R (c.3140A>G) mutation was identified. Such mutations may help predict response to PI3K/mammalian target of rapamycin (mTOR) inhibitors. It has been shown in a variety of non-salivary tumor types that the presence of the PIK3CA p.H1047R mutation was the only independent predictor for tumor response to PI3K pathway inhibitors.
Mutations in EGFR have been reported in 5–9% of SDC. Similarly to lung adenocarcinomas, tumors harboring EGFR mutation may benefit from targeted anti-EGFR therapy. There were no EGFR exons 18, 19, 20, or 21 mutations in our case.
A subset of SDC arising in pleomorphic adenoma is characterized by rearrangements or amplification of pleomorphic adenoma gene 1 (PLAG1) or high mobility group AT-hook 2 (HMGA2) gene. While PLAG1 and HMGA2 alterations are helpful in identifying or confirming the precursor lesion, these are not therapeutically relevant yet.
Supplementary Questions:
- Which of the following parameters is least helpful in assigning pathologic T-Stage to a salivary duct carcinoma?
- Anatomic site
- Facial nerve involvement
- Histologic grade
- Skin involvement
- Tumor size
- Which of the following immunoprofiles is most consistent with salivary duct carcinoma?
- Androgen receptor negative, p63 positive (in all cells)
- Androgen receptor negative, p63 positive (in a subset of neoplastic cells)
- Androgen receptor negative, estrogen receptor positive, progesterone receptor positive
- Androgen receptor positive, prostate specific antigen positive, prostatic acid phosphatase positive
- Androgen receptor positive, p63 negative
- Which of the following genetic alterations currently known to occur in salivary duct carcinoma is of least therapeutic relevance?
- EGFR mutation
- Expression of androgen receptor
- HER2 amplification
- PIK3CA mutation
- PLAG1 rearrangements or amplification
- PTEN deletion
References
- Bahrami A, Perez-Ordonez B, Dalton JD, et al. An analysis of PLAG1 and HMGA2 rearrangements in salivary duct carcinoma and examination of the role of precursor lesions. Histopathology. 2013;63(2):250-262.
- Edge S, Compton CC, Fritz AG, et al. AJCC Cancer Staging Handbook. In: AJCC Cancer Staging Manual. 8th ed. New York, NY. Springer. 2009.
- Griffith CC, Seethala RR, Luvison A, et al. PIK3CA mutations and PTEN loss in salivary duct carcinomas. American J Surg Pathol. 2013;37(8):1201-1207.
- Janku F, Wheler JJ, Westin SN, et al. PI3K/AKT/mTOR inhibitors in patients with breast and gynecologic malignancies harboring PIK3CA mutations. J Clin Oncol. 2012;30(8):777-782.
- Jaspers HC, Verbist BM, Schoffelen R, et al. Androgen receptor-positive salivary duct carcinoma: a disease entity with promising new treatment options. J Clin Oncol. 2011;29(16):e473-476.
- Kaidar-Person O, Billan S, Kuten A. Targeted therapy with trastuzumab for advanced salivary ductal carcinoma: case report and literature review. Med Oncol. 2012;29(2):704-706.
- Nardi V, Sadow PM, Juric D, et al. Detection of novel actionable genetic changes in salivary duct carcinoma helps direct patient treatment. Clin Cancer Res. 2013;19(2):480-490.
- Piha-Paul SA, Cohen PR. Kurzrock, R. Salivary duct carcinoma: Targeting thephosphatidylinositol 3-kinase pathway by blocking mammalian target of rapamycin withtemsirolimus. J Clin Oncol. 2011; 29(26):e727-e730.
Author
2015
Simion I. Chiosea, MD
Surgical Pathology Committee
University of Pittsburgh Medical Center
Pittsburgh, PA
Answer Key
- Histologic grade (c).
- Androgen receptor positive, p63 negative (e).
- PLAG1 rearrangements or amplification (e).