Clinical Summary
A 19-year-old woman presents with abdominal pain and a pelvic mass. Left salpingo-oophorectomy reveals a 1368.0 g, 20.0 x 12.0 x 10.5 cm ovary. Its external surface is smooth and pink without capsular disruption. Sectioning reveals a multiloculated cystic and solid mass. The cyst wall lining is tan-pink, smooth, and ranges from 0.1 to 0.3 cm in thickness. The solid areas are variegated clear, translucent, tan, and dark red with hemorrhage.
Master List
- Carcinosarcoma
- Immature teratoma
- Mature teratoma
- Mixed malignant germ cell tumor
- Primitive neuroectodermal tumor
- Small cell carcinoma in teratoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2013, case 19, and is an immature teratoma.
Criteria for Diagnosis and Comments
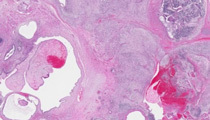
The histologic sections show a mixture of mature tissue derived from all three embryonic layers, including cartilage, bone, epidermis, adnexal structures, respiratory epithelium, and glial tissue. Varying amounts of immature neural tissue are also present in the form of primitive neuroepithelial rosettes and tubules as well as crowded, cellular, mitotically active aggregates of basophilic glial cells. The presence of immature embryonal elements within this ovarian tumor is consistent with the diagnosis of immature teratoma.
Immature teratomas represent approximately 3% of teratomas and roughly 1% of all ovarian malignancies. They generally occur within the first few decades of life and are typically unilateral. Grossly these ovarian tumors are predominantly solid, but may have a cystic component showing hair and sebaceous material typical of a mature teratoma. The solid areas have a variegated, fleshy, grey-tan appearance and may show hemorrhage and necrosis. As with most ovarian tumors, sampling guidelines recommend one section of tumor per centimeter of the maximum tumor diameter; however, as solid teratomas tend to be grossly heterogeneous, more sections may be necessary to sample the tumor adequately. Immature neural elements as described above are the most commonly and reproducibly identified components of immature teratoma, therefore are the only element included in the grading system (see below). Far less commonly seen immature components are loose, myxoid, immature mesenchymal stroma focally differentiating into immature cartilage, adipose, osteoid, or rhabdomyoblasts; immature hepatic tissue or immature renal tissue resembling nephroblastoma are also rarely seen.
For over 50 years, immature teratomas have been graded based on the number of microscopic low power fields (4x) containing immature neuroectodermal tissue present on any one slide. Historically, a three-tiered grading system has been used, defined as follows:
| Grade 1 | Tumor contains less than one low power field of immature neuroepithelium on any one slide. |
| Grade 2 | Immature neuroepithelium occupies greater than one but no more than three low power fields in any slide. |
| Grade 3 | Immature neuroepithelium exceeds three low power fields on any one slide. |
In recent years, a two-tiered grading system (low-grade and high-grade) has been proposed, which is both clinically useful and thought to be more reproducible. As the therapeutic decision to administer chemotherapy in early stage immature teratomas is based on the presence of more than one low power field of immature neural tissue on any one slide (that is, at least grade 2 histology), tumors can be divided into two grades, low and high, with grade 1 histology correlating with low-grade and grades 2 and 3 teratomas comprising high-grade tumors. Low-grade immature teratomas confined to the ovary (stage I) may be managed by resection alone. High-grade tumors require combination chemotherapy, resulting in a cure rate of approximately 95% for stage I disease and 75% for higher stage disease with spread beyond the ovary.
It has been estimated that one-third of immature teratomas have extra-ovarian disease at the time of presentation, most commonly peritoneal implants of either mature or immature tissues. Less commonly, immature teratomas may metastasize to lymph nodes or hematogenously. Adequate sampling and characterization of peritoneal implants is crucial, as immature implants generally require adjuvant chemotherapy, while mature implants (essentially mature glial tissue/gliomatosis) do not warrant chemotherapy. Residual and continued growth of peritoneal disease in the form of benign mature tissue has been reported. These tumors appear to be somewhat resistant to chemotherapy, however are associated with a favorable long-term prognosis when completely surgically resected. Interestingly, although peritoneal gliomatosis of mature tissue is a phenomenon associated with ovarian teratoma, more recent genetic studies have shown these tissues are not derived from the tumor itself, but from metaplasia of pluripotent submesothelial stem cells within the peritoneum, presumably due to growth factors liberated from the teratoma.
In a background of mature elements, thorough sampling revealing a significant immature component will exclude the diagnosis of mature teratoma. Rarely, minute foci of immature tissue in an otherwise typical mature cystic teratoma (dermoid cyst) may be seen; however, these tumors are reported to have a benign clinical course that does not warrant classification as immature teratoma. Care should be taken not to mistake differentiated neural tissue, such as granular cerebellar-type cells, with immature neural elements. In contrast to differentiated neural elements, immature glial foci contain apoptosis and mitotic figures, as well as more vesicular nuclei. Grade 2 and 3 immature teratomas may contain foci of solid overgrowth of neuroectodermal components, which may bring the diagnosis of an ovarian primitive neuroectodermal tumor (PNET) into consideration, particularly since minor foci of bone, cartilage, and rhabdomyoblasts may rarely occur in PNET. However, immature teratomas characteristically show a broad spectrum of neuroepithelial differentiation, as well as a more extensive admixture of endodermal, mesodermal, and other ectodermal tissues. In contrast, an ovarian PNET, which is categorized as a monodermal teratoma, will exhibit massive, confluent growth of neuroectodermal tissue.
Carcinosarcoma of the ovary may be distinguished from immature teratoma by its older age incidence (sixth to eighth decades), rare or only minor component of malignant neuroectodermal tissue, Müllerian-type malignant epithelial component, malignant cartilaginous component with atypical nuclei, and lack of organized tissue units with recognizable fetal structures.
Immature teratomas should be examined closely for the presence of other germ cell tumors such as dysgerminoma or yolk sac tumor. These mixed germ cell tumors account for 10-20% of immature teratomas. The presence and approximate proportions of each component should be reported, although these tumors are all highly responsive to platinum-based chemotherapy.
Secondary carcinoma arising in a teratoma is a well-documented phenomenon. While squamous cell carcinoma and adenocarcinoma are most common, small cell carcinoma occurring within a teratoma has also been reported. Small cell carcinoma of the pulmonary type displays a greater degree of mitotic activity than the immature neuroectodermal tissue it resembles. Additionally, small cell carcinoma is immunoreactive with cytokeratin and TTF1, whereas immature neuroectodermal tissues should be negative for these stains.
Supplementary Questions:
- Immature teratomas are graded based on the quantity of immature mesenchymal tissue present.
- True
- False
- In a patient with a grade 2 immature teratoma confined to the ovary, adjuvant chemotherapy is recommended.
- True
- False
- Immature teratomas have poor overall survival rates.
- True
- False
References
- Crum CP, Nucci MR, Lee KR, eds. Diagnostic Gynecologic and Obstetric Pathology. 2nd ed. Philadelphia, PA: Elsevier Saunders. 2011;930-935.
- Ferguson AW, Katabuchi H, Ronnett BM, Cho KR. Glial implants in gliomatosis peritonei arise from normal tissue, not from the associated teratoma. Am J Pathol. 2001;159:51-55.
- Kwan M, Kalle W, Lau GTC, Chan JKC. Is gliomatosis peritonei derived from the associated ovarian teratoma? Hum Pathol. 2004;35:685-688.
- Nogales F, Talerman A, Kubik-Huch RA, Tavassoli FA, Devouassoux-Shisheboran M. Germ cell tumours. WHO Classification of Tumours. Pathology and Genetics. Tumours of the Breast and Female Genital Organs. Lyon, France: IARC Press; 2003;169-170.
- Norris HJ, Zirkin HJ, Benson WL. Immature (malignant) teratoma of the ovary: a clinical and pathologic study of 58 cases. Cancer. 1976;37:2359-2372.
- O’Connor DM, Norris HJ. The influence of grade on the outcome of stage I ovarian immature (malignant) teratomas and the reproducibility of grading. Int J Gynecol Pathol. 1994;13:283-289.
- Scully RE, Young RH, Clement PB. Tumors of the Ovary, Maldeveloped Gonads, Fallopian Tube, and Broad Ligament. Atlas of Tumor Pathology. 3rd Series, Fascicle 23. Washington DC: Armed Forces Institute of Pathology. 1996;267-272.
- Ulbright TM. Germ cells tumors of the gonads: a selective review emphasizing problems in differential diagnosis, newly appreciated, and controversial issues. Mod Pathol. 2005;18:S61-S79.
Author
2012
Rochelle A. Simon, MD FCAP
Surgical Pathology Committee
Women & Infants Hospital of Rhode Island, Alpert Medical School of Brown University
Providence, RI
Answer Key
- False (b).
- True (a).
- False (b).