Clinical Summary
A 42-year-old woman presents with complaints of abdominal bloating. Bimanual exam reveals a palpable left abdomino-pelvic mass, and CT scan shows a 12.0 cm mass effacing the left ovary. Numerous septations with fluid levels are visualized. At surgery, a multi-lobulated cystic mass is resected with intraoperative rupture revealing jelly-like pinkish cyst contents. A few grossly necrotic areas are seen. No other gross lesions are noted, and on microscopic exam, the other ovary, both fallopian tubes, and uterus are unremarkable. Immunoevaluation reveals the tumor cells to express cytokeratin 7, CA 19.9, and CDX2; they are weakly and focally expressive of cytokeratin 20.
Master List
- Clear cell carcinoma of ovary
- Metastatic mucinous carcinoma
- Metastatic renal cell carcinoma
- Mucinous cystadenocarcinoma of ovary, Grade I
- Mucinous cystadenoma of ovary
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2013, case 11, and is a mucinous cystadenocarcinoma of ovary, Grade I.
Criteria for Diagnosis and Comments
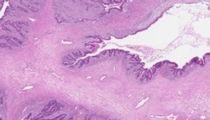
Sections reveal a multicystic neoplasm, with the lumina lined by columnar pinkish cells, approximately 70% of which have cytoplasm distended by mucin. The nuclei are variably located with some being basally located, but in most slides areas show loss of nuclear polarity, nuclear pleomorphism and atypia ranging from mild to marked. In some areas there is evidence of cribriforming. Some, but not all, slides show evidence of a desmoplastic stromal reaction and focal early invasion. The features are those of mucinous cystadenocarcinoma arising in a mucinous cystic neoplasm. It is somewhat unfair to present this tumor as a putative 'one slide' diagnosis in the PIP program for reasons to be discussed below, but a review of the criteria for the diagnosis of ovarian mucinous tumors is felt to be worthwhile.
Mucinous ovarian neoplasms have historically accounted for approximately 15% of ovarian epithelial-stromal tumors. More recent studies, however, suggest their relative incidence is actually less than 10% of lower stage (FIGO Stage I and II) primary ovarian carcinomas and only 1-2% of higher stage (FIGO III and IV) tumors. The reason for the decline in incidence of primary mucinous carcinomas most likely reflects improvement in the ability of pathologists to distinguish primary from metastatic mucinous carcinomas, and the realization over past 15 years than most cases of pseudomyxoma peritonei (PMP) with ovarian involvement actually reflect metastatic disease from an appendiceal tumor. Like their serous counterparts, mucinous tumors can be divided into benign (cystadenomas), 'borderline' (or 'low malignant potential' or 'atypically proliferating—the adjectives are used interchangeably) mucinous tumors, and mucinous cystadenocarcinomas. Grossly the tumors may range from a few millimeters to over 20.0 cm, and they not uncommonly coexist with other ovarian tumors, especially Brenner tumors or teratomas. The vast majority of mucinous primary carcinomas are confined to the ovary at diagnosis. Widely disseminated disease should prompt careful consideration of extra-ovarian origin, most likely in the lower gastrointestinal tract.
Mucinous lesions are notoriously heterogeneous, with many tumors appearing benign through many sections, only to manifest foci of higher grade histology with frankly malignant areas in only a few slides. For this reason, mucinous tumors should be examined with great diligence, and be well sampled for microscopic examination. Recommendations include a submission of one block per centimeter of greatest dimension of the tumor for lesions less than 10.0 cm, and 2 blocks per centimeter for tumors with a greatest dimension greater than 10.0 cm, with attention being paid to solid areas within the tumor, particularly near areas of necrosis. Patients with entirely bland-appearing tumors should undergo long term-clinical follow-up as many may present with recurrent disease years later, even with a diagnosis of mucinous cystadenoma (many of these are probably under-diagnosed carcinomas). Approximately 85% of mucinous tumors exhibit 'intestinal type' histology, with the lining cell reminiscent of gastrointestinal lining cells; the presence of 'goblet cells' is not a requirement. Less than 15% manifest an 'endocervical' type histology reminiscent of endocervical epithelium and tend to be of benign or borderline-type.
Mucinous carcinomas typically show a range of histologic and cytologic findings inclusive of borderline or atypically proliferating neoplasms (stratification of 2-3 cell layers, atypia, mitoses), but additionally have foci of cribriforming, severe nuclear atypia, confluent growth, or frank invasion. 'Invasion' can be manifested by two patterns, which may or may not coexist. The commonest is confluent glandular growth and expansile growth, with minimal intervening stroma, resulting in reticulated or complex patterns. Destructive stromal invasion with a frankly malignant appearance is helpful for diagnosis, but less commonly seen. Invasion of either pattern must exceed 5.0 mm in linear extent or 10.0 mm2 for a diagnosis of 'invasive carcinoma'; otherwise a designation of microinvasion is more appropriate. Foci of anaplastic frankly malignant invasive tumor are more likely to be found in cases with definitive destructive stromal invasion and typically do not present a diagnostic dilemma. The finding of invasive or microinvasive foci should prompt submission of additional sections for histologic examination.
Rare tumors manifest mural nodules, which are solid, cellular areas exhibiting benign or malignant mesenchymal features. Benign nodules may resemble leiomyomas or rhabdomyomas; malignant nodules may suggest chondrosarcoma or other high-grade sarcomas. Immunoevaluation has revealed some of these to be carcinosarcomas or spindle cell carcinomas.
Immunoevaluation of intestinal type mucinous carcinomas reveals tumor cells expressive of cytokeratins 7 and 20, CEA, and CDX2. CA 19.9 is usually strongly positive, and CA-125 is typically not expressed. Molecular studies show high incidence of KRAS mutations, similar to low-grade serous carcinomas of the ovary, but BRAF mutations are unusual. Unlike other ovarian carcinomas, mucinous tumors show no association with BRCA1 or BRCA2 germline or somatic mutations.
The prognosis of primary mucinous carcinomas is generally good for low-grade, low-stage tumors, which constitute the great majority of cases. Recurrences tend to occur most commonly in patients with destructive stromal invasion and usually are localized pelvic disease: when this occurs, the prognosis becomes more ominous. Most patients do not respond well to chemotherapy.
Mucinous cystadenomas show cystic spaces lined by mucinous epithelial cells with a generally banal histologic appearance and constitute the vast majority of mucinous cystic neoplasms (80%). They may be uni- or multilocular but tend toward the latter. Absence of cytologic atypia, mitotic activity, and stratification is a requirement to distinguish cystadenomas from borderline or atypically proliferating mucinous tumors. As emphasized previously, extensive sampling, particularly in larger neoplasms, is essential to exclude foci of de-differentiation. In contradistinction to low and high grade serous tumors, there is reasonably good evidence that mucinous tumors do follow an adenoma-carcinoma continuum sequence, with carcinomas and/or low malignant potential tumors deriving from adenomas.
Metastatic mucinous carcinoma typically derives from the gastrointestinal tract. These tumors are more apt to be bilateral and exhibit other features which provide clues to the metastatic origin, particularly when so-called 'dirty' or 'necklace' type necrosis is seen. The presence of signet ring cells should raise suspicion for a classic 'Krukenberg' tumor (metastatic gastric carcinoma). Whereas bilateral metastatic ovarian carcinomas are often casually referred to as Krukenberg tumors by clinicians, the term should be reserved for metastatic gastric malignancies. Features favoring metastatic origin of mucinous carcinoma in the ovary are summarized below:
- Bilateral ovarian involvement
- Multi-nodular and variable patterns of ovarian involvement
- Microscopic surface implants
- Lymphovascular invasion (especially extra-ovarian or hilar)
- 'Signet ring' forms
- Infiltrative cords and strands of malignant cells
- Cells 'floating' in mucin
- Extraovarian spread
Immunoevaluation will typically show more intense expression of cytokeratin 20, particularly in tumors of colonic origin, than in primary mucinous tumors; but there can be extensive overlap and this marker, alone, may not be an effective discriminator. It is now well-accepted that PMP or diffuse abdominal/peritoneal mucinosis, is a complication of a primary appendiceal mucinous carcinoma. These may also involve the ovary and frequently present as a unilateral or bilateral ovarian masses. The finding of an ovarian mass co-existing with PMP should prompt evaluation of the appendix for a primary tumor site.
Clear cell carcinoma of ovary (CCO) is something of an anomaly in ovarian neoplasia, as most are malignant. CCOs are commonly seen in the 5th decade and later; less than 10 percent appear in younger women. Like mucinous tumors, they usually present as unilateral masses and are FIGO stage IA at presentation. Patients present with complaints related to an abdominal mass. Many patients (50-75%) have a history of pelvic endometriosis, with 25% of tumors arising in or near an endometriotic cyst. Research suggests high concentrations of iron may predispose to mutations in one of the 60 or so genes linked to clear cell carcinogenesis. Histologically, CCO is notable for "hobnail cells," which have scant cytoplasm and blunt nuclei protruding into a luminal space; while these may not be seen in all tumors, they are generally absent in mucinous neoplasms. The cytoplasm is typically abundant and optically "clear" giving the eponymous name to the tumor, but some may have a more eosinophilic or granular appearance. Nuclei are pleomorphic, with coarse granular chromatin and variably prominent nucleoli. Cells often manifest solid and papillary growth patterns and some tubulo-cystic areas may simulate rosette formation, which may suggest yolk sac or granulosa cell tumor. Cytokeratins and epithelial membrane antigen will be strongly positive with immunostaining; it is important to remember that CCO may express PLAP, albeit weakly, which may be an additional point of confusion. Approximately 20% of clear cell carcinomas have a mixed component of endometrioid carcinoma, perhaps related to the common association with endometriosis. Grading of CCO has been attempted, but unlike other epithelial ovarian tumors, grade does not correlate with prognosis, and all are considered high-grade neoplasms. Prognosis for CCO is stage-dependent, with FIGO stage I tumors yielding 15–30% mortality at 5 years; 70–100% of patients with stage III or IV succumb to their disease in the same interval. CCO responds best to chemotherapy regimens including cisplatin and paclitaxel, with cytoreductive surgery, but stage for stage, CCO has a more ominous prognosis than mucinous or other ovarian carcinomas.
Metastatic renal clear cell carcinoma (RCC) has aggregates of optically clear cells which may be columnar in areas, and may rarely have mucinous-type foci, but it manifests a prominent sinusoidal vascular network not seen in mucinous tumors and does not elaborate abundant mucin. The clinical history of a renal mass should assist in diagnosis. Should a RCC announce itself by ovarian metastasis, the tumor will not express the immunomarkers typical of a mucinous neoplasm; renal carcinomas are typically CK7, CK20 negative and express RCC antigen; about 50% will be EMA positive. RCC is not amenable to chemotherapy and patients who present with ovarian involvement obviously have advanced stage disease, and the ultimate prognosis is poor.
Supplementary Questions:
- Which finding gross or microscopic finding is least suggestive of extra-ovarian origin for an ovarian mucinous tumor?
- Bilateral masses
- Foci of necrosis
- Signet ring cells
- Unilateral mass
- Which antibody or molecular finding is not typical of primary ovarian mucinous carcinoma?
- Expression of CDX2
- Expression of cytokeratin 7
- Presence of BRCA-1 or BRCA-2 mutations
- Presence of KRAS mutations
- Which of the following neoplasms is commonly found in association with an ovarian mucinous tumor?
- Brenner tumor
- Leiomyoma
- Mesonephric duct remnant
- Serous cystadenoma
References
- McCluggage, G. Morphological subtypes of ovarian carcinoma: a review with emphasis on new developments and pathogenesis. Pathology 2011; 43(5):420-432.
- Nucci MR, Oliva E. Gynecologic Pathology. New York, NY: Churchill Livingstone Elsevier; 2009.doi:10.1186/1476-4598-6-12.
- Takano M, Kikuchi Y, Yaegashi N, et al. Clear cell carcinoma of the ovary: a retrospective multicentre experience of 254 patients with complete surgical staging. Br J Cancer. 2006;94:1369-1374.
- Wiegand KC, Shah SP, Al-Agha OM, et al. ARID1A mutations in endometriosis-associated ovarian carcinomas. N Engl J Med. 2010;363:1532-1543.
Author
2012
Philip A. Branton, MD FCAP
Surgical Pathology Committee
National Cancer Institute
Rockville, MD
Answer Key
- Unilateral mass (d).
- Presence of BRCA-1 or BRCA-2 mutations (c).
- Brenner tumor (a).