Clinical Summary
A 24-year-old woman presents with abdominal fullness and a palpable mass on bimanual exam. Imaging reveals a solid mass in the left ovary. Non-enhancing magnetic resonance imaging (MRI) shows high signal intensity centrally with a decreased peripheral signal. At laporatomy, a grey-white bosselated mass with a smooth surface is removed by enucleation. The tumor is yellow-white on sectioning and is largely solid with a few small cystic areas. It measures 12 x 10 x 7 cm in maximum dimensions.
Master List
- Brenner tumor
- Fibroma
- Granulosa cell tumor, adult type
- Krukenberg tumor
- Sclerosing stromal tumor
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2015, case 11, and is a sclerosing stromal tumor.
Criteria for Diagnosis and Comments
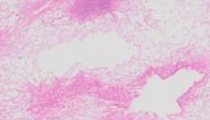
On microscopic examination, the mass appears biphasic at lower power, with more solid-appearing cellular areas irregularly interspersed with hypocellular, edematous or collagenous-appearing zones. This imparts a vaguely lobulated appearance to the tumor. Some sections may retain a rim of compressed, normal ovarian parenchyma. A prominent fine vascular network is visible and surrounds, in the more cellular areas, spindled bland cells with elongated nuclei and oval nuclei intermingled with more oval luteinized cells. The latter have eosinophilic cytoplasm, which may contain vacuoles suggestive of signet-ring cells. Mitotic activity is absent and there is no cytologic atypia. The histologic appearance and clinical features are classic for a sclerosing stromal tumor (SST).
SST is one of the less common sex cord-stromal tumors (2-5% of stromal tumors) and quite rare in the pantheon of ovary neoplasms generally (<1%). First described by Scully in 1973, a SST typically presents as a unilateral ovarian mass in a young woman in the second and third decades. Many tumors ‘self- enucleate’ at surgery due to their circumscribed nature, as did the tumor in this example. Ascites is uncommon, as is hormonal production, and most clinical symptoms derive simply from the presence of a localized pelvic mass. Immunoevaluation typically reveals strong reaction to calretinin and smooth muscle actin antibodies, with widely variable expression of inhibin. Most tumors express estrogen and progesterone nuclear receptors but do not express epithelial antigens such as cytokeratins or epithelial membrane antigen. Molecular analyses in sex cord stromal tumors have tended to focus on more common variants such as granulosa cell tumors and fibromas; trisomy 12, trisomy 14 and monosomy 22 tend to predominate. In the few cases of SST evaluated, there has been a tendency toward trisomy 12 but no unique diagnostically or prognostically useful findings have been reported to date. The diagnosis is typically made based on clinical, histologic, and immunohistochemical findings. Surgical removal is adequate treatment and the prognosis is excellent.
Brenner tumors (transitional cell tumors) of the ovary are relatively rare (1-2% of all ovarian tumors), epithelially-derived, benign solid neoplasms which typically afflict women in the middle to later decades. Origin from Walthard or urothelial ovarian surface rests has been postulated. They are generally asymptomatic other than the presence of a localized mass and may be discovered incidentally. Grossly, the lesions are circumscribed, grey-white solid masses with a dull grey cut surface and are less than 5.0 cm in size. Approximately 5% of cases are bilateral. Microscopic examination reveals a biphasic tumor with dense fibrous stroma surrounding islets of transitional or urothelial-type epithelial cell aggregates, which are of variable frequency from tumor to tumor and may exhibit cystic changes. Calcifications are not uncommon. As with other epithelial tumors, atypically proliferating or low malignant potential forms have been described (1-2% of all transitional tumor cases) and, even more rarely, malignant case examples are in the literature. Brenner tumors frequently co-exist (20-30%) with other primary ovarian neoplasms, especially mucinous and teratomatous tumors. Surgical excision is adequate treatment with no risk of long-term morbidity or mortality.
Fibromas have many similarities to SST, and are composed of bland spindled cells with variably hyalinized areas, but they lack the edematous zones and typically do not contain rounded cells with cytoplasmic vacuoles. Clinically, fibromas appear in an older age group, after the 4th or 5th decades; smaller examples are often found incidentally; but larger tumors (greater than 6.0 cm) are associated with ascites and/or Meig syndrome. Fibromas typically stain weakly and focally for calretinin and inhibin; vimentin is strongly positive. A subset of patients with multiple fibromas have Gorlin syndrome, caused by a mutational inactivation of the PTCH gene. These patients classically present in younger decades, with multiple basal cell carcinomas, odontogenic keratocysts, and palmoplantar pitting. The vast majority of fibromas are sporadic and not associated with Gorlin syndrome. Like SST, fibromas are not hormonally active and most are unilateral except for Gorlin-associated tumors. The major clues in differentiating fibroma from SST are the age of the patient and the absence of the vague lobulated appearance fostered by the edematous zones described above. In addition, fibromas typically lack the cellular heterogeneity and prominent vascularity characteristic of SST. Like SSTs, fibromas are benign and excision is adequate treatment, with an excellent long-term prognosis.
Granulosa cell tumors (GCTs) constitute 1-2% of all ovarian tumors and are typically highly cellular. The constituent cells contain oval nuclei with a linear groove said to resemble a coffee bean. Solid, cystic, and trabecular patterns are common, frequently in the same neoplasm. A minority of tumors will at least focally manifest Call-Exner follicles with the cells arrayed about a central lumen containing eosinophilic secretions, and some may undergo partial hyalinization. Most granulosa cell tumors are hormonally active with secretion of estrogen. While most patients are past the 2nd decade at presentation, cases in children occur and the hyper-estrogenic state stimulates precocious puberty. In older patients, metrorrhagia is typical, with endometrial hyperplasia or endometrioid carcinoma leading to a diagnostic workup and discovery of the ovarian mass. Approximately 20% of granulosa cell tumors recur locally, notoriously many years after the intial presentation; occasional tumors may behave aggressively with metastasis and death; these are typically larger, with high mitotic indices and nuclear atypia. As with other sex cord stromal tumors, GCTs tend to express inhibin and calretinin. The risk for late recurrence decades after presentation mandates prolonged clinical follow-up with regular pelvic imaging and serologic assessment for inhibin. GCTs lack the spindled cells and delicate vascular network typical of SSTs, a point to consider in tumors with extensive hyalinization; in those tumors with Call-Exner follicles the diagnosis is easy. The less-common “juvenile” granulosa cell tumors are not restricted to children, nuclei are more hyperchromatic, lack the classic nuclear grooves, and when cystic tend to have more irregularly-shaped and sized lumina. Trisomy 12 is a common molecular finding, as with adult GCTs, and like more common adult variants, juvenile GCTs express inhibin and calretinin.
Krukenberg tumor classically refers solely to metastatic signet ring cell carcinoma of gastric origin, and like most metastatic carcinomas to the ovary, is bilateral on presentation. The patients are typically in the 5th decade or older; in some patients this is the primary presentation of the disease, with the gastric primary carcinoma being discovered after the ovarian metastases. The lower power appearance may deceptively mimic SST with more solid, fibrous areas commingling with edematous zones. Higher power examination reveals the often-subtle infiltrating signet ring cells, with bland, compressed nuclei in cells with cytoplasmic vacuoles deforming the nucleus. PAS cytochemical stain and CK 7 immunostain typically will highlight the tumor cells. The long-term prognosis of patients with Krukenberg tumor is extremely poor and most patients succumb to widespread metastatic carcinoma.
Supplementary Questions:
- Which of the following is correct regarding the vacuolated cells in sclerosing stromal tumors (SST)?
- The intense expression of CA-125 is diagnostic for SST.
- They exhibit trisomy 12, a unique marker for SST.
- They only express epithelial markers.
- They typically express calretinin and variably express inhibin.
- They uniquely co-express calretinin and epithelial markers.
- Which of the following can be associated with a syndrome including multiple basal cell carcinomas, odontogenic keratocysts, and palmar pitting?
- Adult granulosa cell tumor
- Brenner tumor
- Fibroma
- Krukenberg tumor
- Sclerosing stromal tumor
- Which of the following statements regarding Krukenberg tumors is true?
- Most patients are in the second or third decades.
- The signet ring cells are paradoxically negative for cytokeratins.
- The term refers to metastatic carcinomas of colonic origin.
- They are typically bilateral.
- They are typically unilateral.
References
- Chalvardjian A, Scully R. Sclerosing stromal tumors of the ovary. Cancer. 1973;31(3):664-670.
- Oliva E, Nucci MR. Gynecologic Pathology. New York, NY: Churchill Livingstone/Elsevier. 2009; 457-468,436-441.
- Roth LM. Recent advances in the pathology and classification of ovarian sex cord-stromal tumors. Int J Gyn Pathol. 2006;25(3):199-215.
- Yan Fang L, Jin-Cheng Z, Jian-Bo R et al. Ovarian sclerosing stromal tumor in a young woman with ectopic pregnancy: clinical, pathological, and immunohistochemical studies. Int J Clin Exp Pathol. 2014;7(1):456-459.
Author
Philip A. Branton, MD
Surgical Pathology Committee
National Cancer Institute,
Rockville, MD
Answer Key
- They typically express calretinin and variably express inhibin. (d)
- Fibroma. (c)
- They are typically bilateral. (d)