Clinical Summary
A 70-year-old woman presents with a 7.0 cm right supraclavicular neck mass, night sweats, fatigue, and an unintentional 10-pound weight loss. There are no overlying skin changes. Radiologic imaging studies reveal a complex mass separate from the normal right thyroid lobe. Fine-needle aspiration and core biopsy reveal a high-grade malignant neoplasm with the following immunoprofile: cytokeratin CAM5.2+ (focal), desmin+ (focal), thyroglobulin-, TTF-1-, PAX-8-, HMB45-, Melan A-, S100-, synaptophysin-.
The patient starts neoadjuvant chemoradiotherapy and has minimal response over three months; surgical debulking is performed (the mass is not completely resected due to encasement of carotid artery). Minute foci of papillary thyroid carcinoma are identified in two lymph nodes (without extranodal extension). Otherwise, the entire right neck mass is represented by a high-grade spindle cell neoplasm. At the closest point, the metastatic conventional papillary thyroid carcinoma is about 0.6 cm from the high-grade spindle cell component. Normal thyroid, thymic, or salivary tissue is not identified in the specimen.
Master List of Diagnoses
- Anaplastic thyroid carcinoma with heterologous differentiation (leiomyosarcoma)
- Leiomyosarcoma with non-specific cytokeratin staining
- Malignant melanoma
- Medullary thyroid carcinoma
- Poorly differentiated thyroid carcinoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2016, case 33, and is an anaplastic thyroid carcinoma with heterologous differentiation (leiomyosarcoma).
Criteria for Diagnosis and Comments
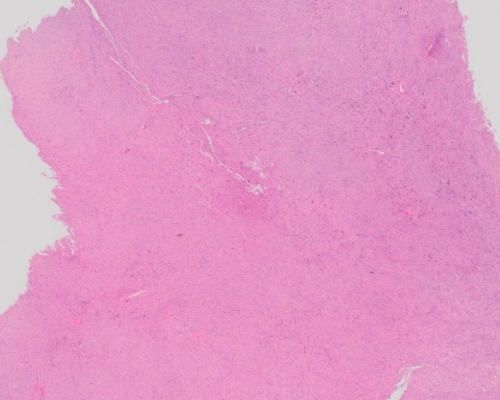
The histological sections reveal spindled cells with bizarre enlarged pleomorphic nuclei with coarse chromatin and prominent pink nucleoli. Some cells are multinucleated. A subset of cells has abundant eosinophilic cytoplasm with filamentous material highlighted by desmin. Occasional eccentric eosinophilic cytoplasmic inclusions are present. In the background, there are numerous inflammatory cells, including histiocytes, eosinophils, and neutrophils. Necrosis and apoptotic debris can be appreciated. In sections with soft tissue, the neoplasm infiltrates through normal adipose tissue. Otherwise, relationship to adjacent normal tissue and organs (eg, thyroid, thymus) is uncertain. Thyroid follicle formation and colloid production are absent. The overall histopathologic features are those of a high-grade malignancy but are non-specific.
The identification of a well-differentiated papillary thyroid carcinoma (PTC) component intermingled with higher grade component is usually the most helpful finding in diagnosing an anaplastic thyroid carcinoma (ATC). The presence of the well-differentiated PTC component is also most reliable in excluding primary or metastatic non-epithelial neoplasms. In this case, extensive sampling revealed metastatic well-differentiated PTC, up to 0.9 cm, confined to two cervical lymph nodes; however, the predominant high-grade component was not admixed with the well-differentiated PTC. The exclusive extrathyroidal presentation of ATC with clinically occult primary thyroid focus is also very unusual. To address the possibility of an ATC (rather than a sarcoma co-existing with an unrelated metastatic PTC with occult primary), molecular testing was performed on conventional PTC and high-grade spindle cell components. Both components were shown to carry BRAF p.V600E mutation, while only the high-grade component was found to harbor TP53 p.R248Q mutation. Overall, given the apparent common clonal origin, this tumor is best designated as an ATC. The presence of the TP53 mutation suggested progression of the PTC into the ATC.
When compared to ATC, poorly differentiated thyroid carcinomas are characterized by a combination of solid, insular, and trabecular architecture, monotonous and smaller cells, punctate necrosis, and retained expression of cytokeratins and TTF-1. Most commonly, the progression of well-differentiated PTC into a poorly differentiated thyroid carcinoma is accompanied by the partial or complete loss of thyroglobulin expression and most poorly differentiated thyroid carcinomas and ATCs show no or weak and focal thyroglobulin expression. While TTF-1 and TTF-2 are rarely expressed in ATC, PAX-8 immunohistochemistry is positive in about 70% of ATC.
The immunoprofile of the neoplasm argues against the diagnosis of a melanocytic neoplasm (negative HMB45, Melan A, S100) or medullary thyroid carcinoma (negative synaptophysin). While BRAF mutations are common in melanocytic and follicular thyroid neoplasms, BRAF mutations are not reported in medullary thyroid carcinomas.
This patient was placed on palliative therapy with selective BRAF inhibitor (vemurafenib) and, initially, continued to have a stable disease. After two months of therapy the patient developed transaminitis (elevated liver enzymes) and QT prolongation as identified by electrocardiography (most likely due to hypokalemia). For these reasons, vemurafenib was discontinued. The patient died 11 months after presentation.
Other side effects of vemurafenib include skin rash, cutaneous squamous cell carcinomas (cSCC), and arthralgia. Up to 25% of patients treated with vemurafenib develop cSCC, sometimes within eight weeks of starting the therapy. Some patients developed multiple cSCC with the second focus identified just six weeks after the discovery of the first focus. cSCC induced by BRAF inhibitors are managed by surgery alone without treatment interruption.
Supplementary Questions
- Which of the following is characteristic of poorly-differentiated thyroid carcinoma and distinguishes it from an ATC?
- Extensive vascular and perineural invasion
- Monotonous cell population with solid/trabecular growth, punctate necrosis, and immunohistochemical expression of TTF-1
- Prominent extrathyroid extension and distant metastases
- Synaptophysin positivity
- Unequivocal nuclear features of conventional papillary thyroid carcinoma with squamous metaplasia and strong PAX-8 expression
- Which of the following immunohistochemical markers is most commonly positive in ATC?
- Epithelial membrane antigen
- PAX-8
- Thyroglobulin
- TTF-1
- TTF-2
- Which secondary malignancy is most commonly identified in patients receiving BRAF inhibitors?
- Ameloblastoma
- Cutaneous squamous cell carcinoma
- Hairy cell leukemia
- Papillary thyroid carcinoma
- Pulmonary adenocarcinoma
References
- Dobashi Y, Sugimura H, Sakamoto A, et al. Stepwise participation of p53 gene mutation during dedifferentiation of human thyroid carcinomas. Diagn Mol Pathol. 1994;3(1):9-14.
- Hagen B, Trinh VA. Managing Side effects of vemurafenib therapy for advanced melanoma. J Adv Pract Oncol. 2014;5(6):400-410.
- Nikiforova MN, et al. Targeted next-generation sequencing panel (ThyroSeq) for detection of mutations in thyroid cancer. J Clin Endocrinol Metab. 2013;98(11):E1852-1860.
- Volante M et al. Poorly differentiated thyroid carcinoma: the Turin proposal for the use of uniform diagnostic criteria and an algorithmic diagnostic approach. Am J Surg Pathol. 2007;31(8):1256-1264.
Author
2016
Simion I. Chiosea, MD
Surgical Pathology Committee
University of Pittsburgh Medical Center
Pittsburgh, PA
Answer Key
- Monotonous cell population with solid/trabecular growth, punctate necrosis, and immunohistochemical expression of TTF-1 (b)
- PAX-8 (b)
- Cutaneous squamous cell carcinoma (b)