- Home
- Member Resources
- Pathology Case Challenge
- Mesentery
Clinical Summary
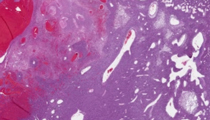
A 60-year-old man presents to the emergency room with a possible appendicitis, with right lower quadrant acute abdominal pain and point tenderness that radiates to the scrotum. Physical exam reveals guarding and rebound tenderness. Peripheral blood examination is normal. Imaging reveals a lobulated hemorrhagic 7.0 cm mesenteric and omental mass with periappendicitis and engorged peripheral vessels; abdominal exploration, mass resection and appendectomy are performed. Gross examination reveals a 7.0 cm lobulated, tan, soft mass of the omentum, mesentery and mesoappendix, with a fleshy cut surface.
Master List
- Dedifferentiated liposarcoma
- Gastrointestinal stromal tumor
- Hemangioma variant
- Mesenchymal chondrosarcoma
- Solitary fibrous tumor
- Spindle cell carcinoma variant
- Synovial sarcoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2013, case 18, and is a solitary fibrous tumor.
Criteria for Diagnosis and Comments
This large 7.0 cm tumor has a lobular growth pattern with a haphazard arrangement of plump spindled cells, stromal and perivascular hyalinization, and a staghorn or hemangiopericytoid vascular pattern. Scattered foci of coagulative necrosis, plump mild to moderate cytologic atypia with pleomorphism, and easily identifiable mitoses are present. By immunohistochemistry, the neoplastic cells are positive diffusely for CD34 and are negative for pankeratins, CD117, S100 protein, desmin, EMA and CD31, supporting solitary fibrous tumor (SFT), low-grade malignant.
Criteria for SFT, low-grade malignant include size greater than 5.0 cm, increased cellularity, cytologic atypia or epithelioid growth pattern, mitoses greater than 4/10 hpf, hemorrhage (particularly subcapsular), infiltrative growth pattern, and geographic necrosis. Not all features need be present to classify as low-grade malignant. For the current case, based on the large size, mitoses, increased cellularity, cytologic atypia, hemorrhage, and necrosis, this would be classified as a low-grade sarcoma, grade 1/3 French Federation of Cancer Centers Sarcoma Group (FNCLCC). More than 70% of SFT overall behave well. While prediction of malignancy can be difficult, specific present criteria, as in the current case, would render the current lesion as having potential low-grade malignant behavior, with low risk for metastasis to lung, bone, liver. Complete (wide) excision is the treatment of choice.
SFT, a specialized CD34-positive fibroblastic tumor, is now combined as an entity with the formerly called "hemangiopericytoma." SFT can occur in many locations with equal sex predilection in 20-70 year old adults and is often low-grade malignant when intrathoracic, intraabdominal, intrapelvic or retroperitoneal. SFT is well known to have several enlarged vessels around it with intralesional vessels demonstrating staghorn architecture and perivascular hyalinization. In intrathoracic locations it can present as a pseudoaneurysm. Compression and hypoglycemia are rare complications. Ophthalmic giant cell angiofibroma is a related entity and sinonasal hemangiopericytoma is an unrelated CD34-negative myopericytic family tumor.
Dedifferentiated liposarcoma may be in the differential diagnosis in this deep mesenteric location and SFT can have intralesional fat; however, there is no adjacent well-differentiated liposarcoma component to the current SFT and the morphology fits better with SFT. Despite CD34 reactivity, this is not a primary vascular neoplasm, excluding hemangioma; additionally, CD31, our best vascular marker, is negative in the tumor cells of SFT. This tumor was originally considered a sarcoma at the time of frozen section; the most common sarcoma of this region would be gastrointestinal stromal tumor yet the absence of serosal involvement, haphazard arrangement of spindled cells, staghorn vasculature and CD117 negativity exclude that entity. Other tumors that do have staghorn vasculature include mesenchymal chondrosarcoma, an S100 protein positive round cell tumor with metaplastic hyaline cartilage (not present here) and synovial sarcoma, which would exhibit cytokeratins and EMA and would be negative for CD34 (not present here). Spindle cell carcinoma is excluded by morphology and absence of keratins. The best diagnosis is SFT.
Supplementary Questions:
- Which tumors can have staghorn vasculature?
- Melanoma, carcinoma, lymphoma
- Merkel cell carcinoma, Ewing, rhabdomyosarcoma
- Mesothelioma
- Prostate adenocarcinoma
- Synovial sarcoma, mesenchymal chondrosarcoma, solitary fibrous tumor
- What are the criteria for low-grade malignancy in solitary fibrous tumor (SFT)?
- Clinically-identifiable lymph node metastasis confirmed by imaging
- Cytologically bland monotonous uniformity
- Focus of lymph node metastasis that can be identified only by CD34 stain
- Large size (>5 cm), mitoses >4/10 hpf, necrosis
- Peripheral location
- Centrally-located SFT have more likelihood of low-grade malignant behavior.
- True
- False
References
- Furusato E, Valenzuela IA, Fanburg-Smith JC, et al. Orbital solitary fibrous tumor: encompassing terminology for hemangiopericytoma, giant cell angiofibroma, and fibrous histiocytoma of the orbit: reappraisal of 41 cases. Hum Pathol. 2011;42(1):120-128.
- Lee JC, Fletcher CD. Malignant fat-forming solitary fibrous tumor (so-called "lipomatous hemangiopericytoma"): clinicopathologic analysis of 14 cases. Am J Surg Pathol. 2011;35(8):1177-1185.
- Mosquera JM, Fletcher CD. Expanding the spectrum of malignant progression in solitary fibrous tumors: a study of 8 cases with a discrete anaplastic component-is this dedifferentiated SFT? Am J Surg Pathol. 2009;33(9):1314-1321.
- Zafar H, Takimoto CH, Weiss G. Doege-Potter syndrome: hypoglycemia associated with malignant solitary fibrous tumor. Med Oncol. 2003;20(4):403-408.
- Zong L, Chen P, Wang GY, Zhu QS. Giant solitary fibrous tumor arising from greater omentum. World J Gastroenterol. 2012;18(44):6515-6520.
Author
2012
Julie C. Fanburg-Smith, MD, FCAP
Surgical Pathology Committee
Sibley Memorial Hospital of Johns Hopkins Medicine
Washington DC
Answer Key
- Synovial sarcoma, mesenchymal chondrosarcoma, solitary fibrous tumor (e).
- Large size (>5 cm), mitoses >4/10 hpf, necrosis (d).
- True (a).