- Home
- Member Resources
- Pathology Case Challenge
- Mediastinum
Clinical Summary
A 3-year-old girl presents with an incidental posterior mediastinal mass. The surgically resected mass consists of fragmented and emulsified grey-tan, rubbery tissue measuring in aggregate approximately 8.0 × 7.0 × 7.0 cm, and weighing 54 gm. No capsule or areas of necrosis or hemorrhage are identified grossly. Representative sections of the resection specimen are analyzed for histologic analysis.
Master List
- Ganglioneuroblastoma
- Ganglioneuroma
- Neurofibroma
- Schwannoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2015, case 07, and is a ganglioneuroma.
Criteria for Diagnosis and Comments
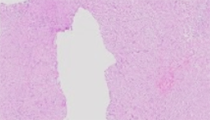
Histologic sections show mature ganglion cells enmeshed within a prominent spindle cell stroma that is derived from mature Schwann cell elements and fibrous tissue. No areas of increased cellularity, cellular atypia, mitoses or necrosis are identified.
Neuroblastoma, ganglioneuroblastoma, and ganglioneuroma are tumors of varying maturity derived from primordial neural crest cells and are referred to collectively as neuroblastic/neurogenic tumors. These primitive sympathetic ganglion cells may remain undifferentiated (neuroblasts) or they may mature (ganglion and Schwann cells). These tumors define a spectrum of sympathetic neuroectodermal tumors; a tumor composed primarily of neuroblasts is referred to as neuroblastoma, a tumor composed entirely of mature ganglion cells and other mature tissue is a ganglioneuroma, and a tumor with both immature and mature cell types is a ganglioneuroblastoma. The biologic behavior of these tumors is generally dictated by the level of maturation and degree of differentiation of sympathetic elements. Consequently, these neuroblastic tumors vary widely in their biologic behavior. The presence of immature tissue in neuroblastoma and ganglioneuroblastoma indicates malignant or potentially malignant behavior. The lack of these immature features is what makes ganglioneuromas benign. Neuroblastoma is the most malignant tumor of the three and may exhibit quite diverse clinical behavior including spontaneous regression, maturation to benign ganglioneuroma, or aggressive metastatic dissemination leading to death. Features such as DNA content, proto-oncogenes, and catecholamine synthesis can influence prognosis and their presence or absence aids in categorizing patients as high, intermediate, or low risk.
Ganglioneuromas may present as a de-novo mass, or they may arise from either, maturing neuroblastomas and ganglioneuroblastomas, or from neuroblastomas that were treated with chemotherapy. The relative frequency of spontaneously occurring ganglioneuromas, ganglioneuroma arising from maturing neuroblastomas and ganglioneuroblastoma, and ganglioneuromas arising from treated neuroblastomas and ganglioneuroblastoma is currently unknown. There are rare reports of metastatic ganglioneuromas. However, it is believed that these tumors likely represent metastases of neuroblastomas or ganglioneuroblastoma that have subsequently matured to ganglioneuromas and, as such, these patients have an excellent prognosis.
Grossly, ganglioneuromas average 8.0 cm in greatest diameter and often appear as a well-circumscribed, firm, relatively homogeneous, encapsulated mass. These tumors arise wherever sympathetic tissue exists. The most common locations are the posterior mediastinum (41.5% of cases), retroperitoneum (37.5%), adrenal gland (21%), and neck (8%). They are often fleshy tan to yellow in color, and cut surface may appear trabeculated or whorled. Hemorrhage and necrosis are typically not present. The median age at diagnosis is approximately 7 years, with different studies reporting a median age of 5.5 years, 7 years, and over 10 years. There is a slight female predominance, ranging from 1.13:1 to 1.5:1.
Histologically, ganglioneuromas are composed of mature ganglion cells enmeshed within a prominent spindle cell stroma that is derived from mature Schwann cell elements and fibrous tissue. By definition, ganglioneuromas contain no immature elements such as neuroblasts or intermediate cells. Additionally, cellular atypia, mitotic activity, and necrosis are not histologic features of ganglioneuromas. The presence of immature neuroblasts indicates that the tumor is a ganglioneuroblastoma or neuroblastoma, thereby effectively excluding the diagnosis of ganglioneuroma. Lesions containing only a few isolated immature cells are considered by some to be “maturing ganglioneuromas”.
Clinically, ganglioneuromas most often manifest as an asymptomatic mass discovered on a routine radiographic study. Occasionally ganglioneuromas may cause local mass effect and patients can present with cough, abdominal pain, or dyspnea. In rare cases, ganglioneuromas secrete sufficient quantities of homovanillic acid (HVA) and vanillylmandelic acid (VMA) to manifest with flushing and other symptoms of catecholamine excess. Catecholamine production by ganglioneuromas was previously believed to be unusual because it was thought that more mature tumors have more mature biologic behavior. However, more recent case studies on patients with ganglioneuromas have found that up to 37% of the patients had elevated circulating VMA or HVA levels. Although elevated catecholamine production occurs in 90%–95% of patients with the more immature neurogenic tumors (neuroblastomas and ganglioneuroblastomas), elevated levels may also be seen in ganglioneuroma and therefore cannot be used exclusively to discriminate among neuroblastomas, ganglioneuroblastomas, and ganglioneuromas.
Once a diagnosis of ganglioneuroma is made, treatment consists of complete surgical resection whenever possible. Patient survival and prognosis is excellent, even when complete tumor removal is not possible. Complete resection ensures thorough sampling of the tumor, such that a confident diagnosis of ganglioneuroma can be made. Local recurrence has been reported in the literature, as such, periodic radiologic surveillance is performed after resection.
Immunohistochemically, this family of tumors is characterized by strong expression of neuron-specific enolase (NSE) in the proliferating neuroblastic cells, regardless of differentiation. Staining for neurofilaments has also been demonstrated in gangioneuroma and ganglioneuroblastoma, but this intermediate filament is usually not expressed in neuroblastoma. S100 stains Schwannian stroma but not neuroblastoma cells. Additionally, markers such as chromogranin and synaptophysin can stain the more differentiated cells. A distinguishing feature is neuroblastoma’s lack of reactivity for CD99, a useful finding for differentiating primitive neuroectodermal tumors.
Neurofibromas can also occur in posterior mediastinum in patients with and without NF1 syndrome. These tumors show uniform pattern of bland spindle cells growing in fascicles and storiform arrays with myxoid stroma. Central schwannoma typically show fascicles of spindle cells (Antoni A), without well formed Verocay bodies, and paucity of myxoid areas (Antoni B). There are often also prominent thick walled blood vessels, xanthomatous degeneration and a prominent capsule with pericapsular lymphocytic cuffing.
Supplementary Questions:
- Which of the following is true regarding ganglioneuroma?
- Composed primarily of immature neuroblasts
- Commonly follow a highly malignant and aggressive clinical course
- Grossly present as encapsulated masses with features that include multifocal hemorrhage and necrosis
- May arise from maturing ganglioneuroblastomas or neuroblastomas
- Treatment includes surgery, chemotherapy, and bone marrow transplantation.
- Which of the following most accurately describes the histologic appearance of ganglioneuromas?
- Admixture of neuroblasts and ganglion cells deposited in a fibrillary stroma
- Ganglion cells exhibiting marked cellular atypia, mitotic activity, and tumoral necrosis
- Mature ganglion cells within a fibrous, spindle cell stroma composed of mature Schwann cell elements
- Mixture of mature and immature neuroblasts within a fibrous background with necrosis
- Patchy nodules of immature neuroblasts set within a mature ganglioneuromatous stroma
- Which of the following is true regarding the clinical presentation of ganglioneuromas?
- Always presents with localized mass effect, most often leading to acute respiratory distress symptoms
- At time of diagnosis, will present as primary mediastinal mass as well as multiple metastatic masses throughout the thorax and peritoneum
- Most often presents as an asymptomatic mass discovered on a routine radiograph (chest x-ray)
- Presence of elevated circulating catecholamine levels and symptoms of catecholamine excess will exclude the diagnosis of ganglioneuroma.
- Rapidly enlarging abdominal mass in a newborn
References
- De Bernardi B, Gambini C, Haupt R, et al. Retrospective study of childhood ganglioneuroma. J Clin Oncol. 2008;26:1710.
- Lonerga GJ, Schwab CM, Suarez ES, Carlson CL. Neuroblastoma, ganglioneuroblastoma, and ganglioneuroma: radiologic-pathologic correlation. Radiographics. 2002;22:911-934.
- Meyer S, Reinhard H, Ziegler K, et al. Ganglioneuroma: radiological and metabolic features in 4 children. Pediatr Hematol Oncol. 2002;19:501.
- Weiss SW, Goldblum JR. Enzinger and Weiss’s Soft Tissue Tumors. Fifth ed. Philadelphia, PA: Elsevier; 2008:945-963.
Authors
Joseph Peevey, MD
Pathology Resident
Northwestern University
Chicago, IL
Kirtee Raparia, MD
Surgical Pathology Committee
Northwestern University
Chicago, IL
Answer Key
- May arise from maturing ganglioneuroblastomas or neuroblastomas (d).
- Mature ganglion cells within a fibrous, spindle cell stroma composed of mature Schwann cell elements (c).
- Most often presents as an asymptomatic mass discovered on a routine radiograph (chest x-ray) (c).