Clinical Summary
A 77-year-old man presents with a 5.0 cm nodule on computerized tomography examination. The nodule is partly solid and partly ground glass, located in the periphery of the left lower lobe. The patient has a history of 2.0 cm poorly differentiated, non-small cell carcinoma in the right-upper lobe, which was resected 4 years prior. Gross examination of the left-lower lobectomy specimen reveals an ill-defined, solid mass puckering the overlying pleura. The cut section shows a tan-white, gelatinous, mucoid, lobulated mass measuring 5.0 cm in greatest dimension. Representative sections are submitted for microscopic sections.
Master List
- Invasive mucinous adenocarcinoma/colloid carcinoma
- Mucinous adenocarcinoma in situ
- Mucinous cystadenocarcinoma
- Mucinous minimally invasive adenocarcinoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2015, case 17 and is an invasive mucinous adenocarcinoma/colloid carcinoma.
Criteria for Diagnosis and Comments
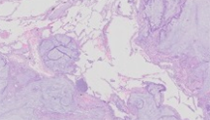
Microscopic sections show tumor cells with abundant intracytoplasmic mucin spreading along the alveolar spaces (lepidic growth pattern). There is mild to moderate cytologic atypia of the tumor cells. Alveolar spaces also contain mucin. Most slides show features of colloid carcinoma; however some slides show definitive areas of invasion with acinar, papillary, and micro-papillary growth patterns. The size of largest focus of invasion measures approximately 8.0 mm. Hence, a diagnosis of invasive mucinous adenocarcinoma is made. The International Association for the Study of Lung Cancer (IASLC)/American Thoracic Society (ATS)/European Respiratory Society (ERS) proposed an International Multidisciplinary Lung Adenocarcinoma Classification in 2011. The new classification has designated mucinous adenocarcinoma in situ as a pre-invasive lesion and recognizes a separate category for mucinous minimally invasive adenocarcinoma. Invasive mucinous adenocarcinoma and colloid carcinoma are described as variants of invasive adenocarcinoma.
Adenocarcinoma in situ (AIS), formerly known as bronchioloalveolar carcinoma (BAC) is a localized small (less than 3.0 cm) lesion with tumor growth restricted to preexisting alveolar spaces (lepidic growth), lacking stromal, vascular, or pleural invasion. In AIS, papillary or micropapillary patterns and intraalveolar tumor cells should be absent. AIS can be of nonmucinous and mucinous types, although most AIS are of nonmucinous type. Mucinous AIS consist of tall columnar cells with basal nuclei and abundant cytoplasmic mucin; sometimes resembling goblet cells. Several studies on solitary lung adenocarcinomas with pure lepidic growth, smaller than 3.0 cm have documented 100% disease-free survival.
Minimally invasive adenocarcinoma (MIA) are also small, solitary tumors (less than 3.0 cm), with a predominantly lepidic pattern and less than 5 mm invasion in greatest dimension in any one focus. MIA is usually nonmucinous but rarely may be mucinous type. The invasive component to be measured in MIA is defined as histological subtypes other than a lepidic pattern (i.e., acinar, papillary, micropapillary, and/or solid) or tumor cells invading the surrounding stroma. These tumors should not have lymphovascular or pleura invasion or tumor necrosis. Studies have also shown 100% disease-free survival in patients presenting with these tumors.
Colloid adenocarcinoma of the lung typically shows pools of extracellular mucin, which distend alveolar spaces causing destruction of their walls. The mucin pools contain clusters of mucin-secreting tumor cells, which may comprise only a small percentage of the total tumor and, thus, be inconspicuous. Colloid adenocarcinoma is often found as a mixture with other subtypes of adenocarcinoma rather than as a pure pattern. A tumor is classified as a colloid adenocarcinoma when it is the predominant component; the percentages of other components should be noted.
Tumors formerly classified as “mucinous cystadenocarcinoma” are very rare, and they probably represent a spectrum of colloid adenocarcinoma. These tumors typically show uni- or oligolocular cystic structures by imaging and/or gross examination. The cysts are filled with mucin and lined by goblet or other mucin-secreting cells with minimal cytologic atypia. The lining epithelium may be discontinuous and replaced with inflammation including a granulomatous reaction or granulation tissue. According to the recent adenocarcinoma classification, these tumors should be included in the category of colloid adenocarcinoma and a comment could be made that the tumor resembles formerly classified mucinous cystadenocarcinoma.
Mucinous tumors of lung have strong tendency for multicentric, multilobar, and bilateral lung involvement, which may be because of the frequent aerogenous spread of the tumor cells. Mixtures of mucinous and nonmucinous tumors may rarely occur. If there is at least 10% of each component, it should be classified as “mixed mucinous and nonmucinous adenocarcinoma.”
Mucinous adenocarcinoma of lung has major clinical, radiologic, pathologic, and genetic differences from the nonmucinous tumors. Mucinous adenocarcinomas usually have strong correlation with KRAS mutation, whereas nonmucinous adenocarcinomas are more likely to show EGFR mutation and rarely KRAS mutation. Studies suggest that KRAS mutations are found in 17-37% of Caucasians and 5-17% of Asian patients with lung adenocarcinomas. KRAS mutations are more frequently found in patients with heavy tobacco exposure, but are also occasionally encountered among never-smokers with lung cancer. These mutations are shown to be associated with advanced tumor progression, and thus suggesting a tendency towards a more aggressive clinical course and shortened patient survival.
IASLC/ATS/ERS Classification of Lung Adenocarcinoma in Resection Specimens
Preinvasive lesion
- Atypical adenomatous hyperplasia
- Adenocarcinoma in situ (≤ 3 cm formerly BAC)
- Nonmucinous
- Mucinous
- Mixed mucinous/nonmucinous
Minimally invasive adenocarcinoma (≤3 cm lepidic predominant tumor with ≤5 mm invasion)
- Nonmucinous
- Mucinous
- Mixed mucinous/nonmucinous
Invasive adenocarcinoma
- Lepidic predominant (formerly nonmucinous BAC pattern, with ≤5 mm invasion)
- Acinar predominant
- Papillary predominant
- Micropapillary predominant
- Solid predominant with mucin production
Variants of invasive adenocarcinoma
- Invasive mucinous adenocarcinoma (formerly mucinous BAC)
- Colloid
- Fetal (low- and high-grade)
- Enteric
(Reference 3) BAC, bronchioloalveolar carcinoma; IASLC, International Association for the Study of Lung Cancer; ATS, American Thoracic Society; ERS, European Respiratory Society.
Supplementary Questions):
- Which of the following is true regarding Mucinous Adenocarcinoma in SITU?
- Acinar and papillary patterns are frequently seen.
- No pleural or lymphovascular invasion is identified.
- Patients with these tumors usually carry a worse prognosis.
- Tiny foci of stromal invasion can be seen.
- Tumor size should be greater than 3.0 cm.
- Which feature is definitive in separating invasive Mucinous Adenocarcinomas from Mucinous Minimally Invasive Adenocarcinoma?
- Imaging of the tumor
- Mitotic activity
- Nuclear pleomorphism
- Size of the invasive focus (should be more than 5.0 mm)
- Size of tumor
- What is the most common mutation seen in patients with mucinous tumors of the lung?
- ALK rearrangement
- EGFR
- KRAS
- p53
- PTEN
References
- Guan JL, Zhong WZ, An SJ, et al. KRAS mutation in patients with lung cancer: a predictor for poor prognosis but not for EGFR-TKIs or chemotherapy. Annals of surgical oncology. 2013; 20(4):1381-1388.
- Kadota K, Yeh YC, D'Angelo SP, et al. Associations between mutations and histologic patterns of mucin in lung adenocarcinoma: Invasive mucinous pattern and extracellular mucin are associated with KRAS mutation. Am J Surg Pathol. 2014; 38(8):1118-1127.
- Travis WD, Brambilla E, Noguchi M, et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J Thorac Oncol. 2011;6(2): 244-285.
Author
Kirtee Raparia, MD
Surgical Pathology Committee
Northwestern University
Chicago, IL
Answer Key
- No pleural or lymphovascular invasion is identified. (b)
- Size of the invasive focus (should be more than 5.0 mm) (d)
- KRAS (c)