Clinical Summary
A 60-year-old man with a 50 pack-year smoking history presents with complaints of persistent cough and pleuritic chest pain. Radiographs demonstrate a 2.5 cm solid, subpleural lesion with spiculated borders involving the left upper lobe. Following a diagnostic needle core biopsy, a lobectomy is performed. The external surface is remarkable for puckering of the pleura. Sectioning reveals a yellow-tan lesion beneath the area of puckering. The provided section is from the tumor. The patient additionally has metastatic disease in mediastinal lymph nodes and 5 months following surgery is discovered to have liver and adrenal metastases.
Master List
- Adenocarcinoma in situ
- Adenocarcinoma, predominantly acinar type
- Colloid carcinoma
- Invasive mucinous adenocarcinoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2013, case 22, and is adenocarcinoma, predominantly acinar type.
Criteria for Diagnosis and Comments
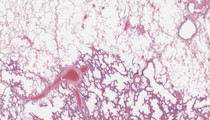
The provided sections demonstrate an invasive, non-mucinous adenocarcinoma of the lung with a wide range of histologic growth patterns. Most of the sections show a predominance of invasive glandular structures set in a fibrotic stroma. Taken in totality, the tumor is best classified as adenocarcinoma, predominantly acinar type. As lung carcinomas are characteristically heterogeneous, some sections may show lepidic or papillary growth or a combination of patterns.
In 2011, an updated classification of pulmonary adenocarcinoma was issued jointly by the International Association for the Study of Lung Cancer (IASLC), the American Thoracic Society (ATS) and the European Respiratory Society (ERS). This classification is presented in the list below. Major changes from the 2004 WHO classification are discussed herein and the reader is directed to the 2011 reference below by Travis, et al. for greater detail.
In this revised classification, a major update is the introduction of the terms adenocarcinoma in situ (AIS) and minimally invasive adenocarcinoma (MIA). These entities are defined as follows:
AIS: "A localized small (< 3.0 cm) adenocarcinoma with growth restricted to neoplastic cells along preexisting alveolar structures (lepidic growth), lacking stromal, vascular or pleural invasion. Papillary or micropapillary patterns and intra-alveolar tumor cells are absent."
MIA: "A small solitary adenocarcinoma (< 3.0 cm) with a predominantly lepidic pattern and < 5.0 mm of invasion in greatest dimension in any one focus." The invasive component is defined as "1) histologic subtypes other than a lepidic pattern (i.e acinar, papillary, micropapillary or solid) or 2) tumor cells infiltrating a myofibroblastic stroma". It is also stated that a diagnosis of MIA is excluded if the tumor "1) invades lymphatics, blood vessels or pleura or 2) contains tumor necrosis".
It should also be noted that AIS and MIA apply primarily to non-mucinous carcinomas, and mucinous variants, while included as subtypes of AIS and MIA, are exceedingly rare.
A second major change in the IASLC/ATS/ERS classification is modification of the WHO category of "mixed subtype," which comprised roughly 85% of all lung adenocarcinomas and encompassed a wide variety of tumors with variable prognosis. As such, it was recommended that tumors not meeting criteria for AIS or MIA should be categorized by the predominant histologic pattern. Of note, the predominant type is the type most frequently present and may not necessarily comprise greater than 50% of the tumor. Subsequent studies evaluating the prognostic significance of this classification system confirm that the predominant histologic pattern correlates well with survival, with lepidic predominant having the best prognosis, micropapillary and solid predominant the worst, and papillary and acinar predominant in between. It should be noted that most of the data for the updated classification is based on studies of small tumors which would be classified as pT1, and the significance needs to be better evaluated in larger tumors.
Mucinous tumor classification is also modified. Multiple studies have shown that the vast majority of tumors previously classified as mucinous bronchioloalveolar carcinoma in fact contain areas of invasion. As such, while very rare mucinous tumors may meet criteria for AIS or MIA, the majority of tumors formerly categorized as mucinous BAC would currently be classified as invasive mucinous adenocarcinoma. Such tumors are comprised of columnar mucinous cells with minimal cytologic atypia. The cells may have either tall columnar morphology with prominent apical mucin or a goblet cell appearance. Colloid carcinoma differs histologically from invasive mucinous carcinoma in that the tumor is characterized by dissecting pools of mucin with free floating tumor cells, similar to its counterparts in breast and colon. Finally, enteric carcinoma, a form of lung carcinoma with histologic and immunohistochemical findings overlapping with colorectal carcinoma, has been formally included in the 2011 classification. It is recommended that at least 50% of the tumor show evidence of enteric differentiation prior to classifying a tumor in this fashion.
The 2011 classification is not without issues that need further validation and study. Chief among these is the issue of staging, as AIS and MIA are not included in the recently released 7th edition of the AJCC staging manual. Additionally, more study is needed in order to determine whether lung carcinomas should be staged by the size of the invasive tumor and/or whether all lepidic growth represents in situ carcinoma.
Reproducibility of the classification system is generally good for certain individual patterns but is only fair overall, with a kappa value of 0.4 in one study undertaken by a large group comprised exclusively of pulmonary pathologists. Major areas of difficulty include identification of stromal invasion in tumors with lepidic growth and discrimination between lepidic and papillary/micropapillary growth. Lepidic growth consists of malignant, but typically cytologically bland, cells growing along pre-existing alveolar structures and, while interstitial fibrosis and "collapse" of alveoli may occur, lung architecture should appear essentially preserved. Clues to discriminating invasive tumor from tumor entrapped in "collapsed" alveoli include angulation of glands, increased nuclear atypia and presence of desmoplastic stroma. Papillary and micropapillary growth are not infrequently mistaken for lepidic growth as the tumor appears within airspaces rather than exhibiting more typical stromal invasion. True lepidic growth should be essentially flat with minimal or no intra-alveolar tumor cells. Papillary growth is characterized by branching papillary structures with fibrovascular cores. In spite of the lack of typical stromal invasion, normal lung architecture is lost, a feature that is often better appreciated on low power. Micropapillary carcinoma is characterized by tufts of tumor cells radiating from a fibrotic core, essentially identical to micropapillary carcinoma described in other organs such as breast or bladder. The micropapillary tufts are generally found within alveolar spaces, within glandular structures or, less frequently, within retraction spaces in fibrotic stroma.
The fact that this patient has advanced disease raises the important issue of molecular testing in lung carcinomas. EGFR tyrosine kinase inhibitors (TKI) such as gefitinib and erlotinib are small molecule competitive inhibitors of EGFR tyrosine kinase, and patients with activating somatic mutations of EGFR, most often of exons 19 and 21, show increased progression free survival following treatment with these agents. Similarly, inversions on chromosome 2p result in creation of an EML4-ALK fusion gene, and the drug crizotinib has provided prolonged disease free survival in patients with tumors containing this translocation, As such, molecular testing is a major issue in patient management. Other "drug-able" mutations such as mutations of BRAF and ROS-1 occur in a small percentage of lung carcinomas and the list of potential targets will continue to expand. The percentage of tumors harboring these mutations is small, generally less than 20% for EGFR mutations, 5-7% for ALK mutations and 1% or less for remaining mutations depending on the study. Currently TKI's and crizotinib are approved only for use in patients with advanced disease outside of clinical trials. Testing recommendations have been issued by the European Working Group, ASCO and other agencies, and a multidisciplinary recommendation drafted jointly by CAP, IASLC and the Association for Molecular Pathology (AMP) is currently in press at the time of this writing. The guidelines recommend testing for adenocarcinomas and mixed lung cancers with an adenocarcinoma component. In excised lung carcinomas, testing is not recommended for tumors that lack any adenocarcinoma component such as "pure squamous cell carcinoma", "pure small cell carcinoma," or large cells carcinomas lacking any immunohistochemical evidence of adenocarcinoma differentiation. The issue of testing early stage disease is also addressed, with much latitude given to the multidisciplinary treatment team and individual patient circumstances. The reader is referred to the reference listed below by Pirker, et al, as well as the forthcoming CAP guidelines for more detailed recommendations, as extensive discussion is beyond the scope of this critique. Important caveats bearing mention include the fact that neither clinical nor histological parameters should be used to direct testing alone. For example, while EGFR mutations are more commonly encountered in tumors occurring in non-smoking Asian females with lepidic or papillary growth, mutations have been reported in tumors occurring in males, smokers and other histologic types of adenocarcinoma, so testing cannot be restricted to a single clinical population. Additionally, while mutation specific immunostains are being developed and show promise in initial studies, the current guidelines recommend that evaluation for EGFR mutations be performed by molecular methods. Detection of increased EGFR copy number by FISH is similarly not recommended due to poorer correlation of response to TKI's in comparison to detection of mutations by molecular analysis. Evaluation for ALK mutations, however, should be performed by FISH analysis based on current recommendations.
2011 IASLC/ATS/ERS classification of pulmonary adenocarcinomas
- Preinvasive lesions
- Atypical adenomatous hyperplasia
- Adenocarcinoma in situ (<3.0 cm formerly BAC)
- Nonmucinous
- Mucinous
- Mixed mucinous/nonmucinous
- Minimally invasive adenocarcinoma (<3.0 cm lepidic predominant tumor with <5.0 mm invasion)
- Nonmucinous
- Mucinous
- Mixed mucinous/nonmucinous
- Invasive adenocarcinoma
- Lepidic predominant (formerly nonmucinous BAC pattern, with >5.0 mm invasion)
- Acinar predominant
- Papillary predominant
- Micropapillary predominant
- Solid predominant with mucin production
- Variants of invasive adenocarcinoma
- Invasive mucinous adenocarcinoma (formerly mucinous BAC)
- Colloid
- Fetal (low and high grade)
- Enteric
Supplementary Questions
- How should most tumors with primarily non-mucinous lepidic growth and a focus of invasive carcinoma measuring <5.0 mm be classified in the IASLC/ATS/ERS classification scheme?
- Adenocarcinoma in situ
- Adenocarcinoma, mixed type
- Adenocarcinoma, predominantly lepidic type
- Atypical adenomatous hyperplasia
- Minimally invasive adenocarcinoma
- Which histologic subtype of adenocarcinoma is associated with the worst prognosis in pT1 tumors?
- Adenocarcinoma, predominantly acinar type
- Adenocarcinoma, predominantly lepidic type
- Adenocarcinoma, predominantly micropapillary type
- Adenocarcinoma, predominantly papillary type
- Minimally invasive adenocarcinoma
- Which of the following statements is true?
- Clinical features alone may be used to select tumors for molecular testing
- EGFR and ALK mutations are present in the majority of lung carcinomas
- EGFR mutations are best detected by immunostaining methods
- Evaluation for ALK mutations should be performed by FISH analysis
- Increased EGFR copy number correlates with response to TKI therapy better than detection of mutations by molecular methods
References
- Ladanyi M, Cagle PT, Lindeman N, et al. Molecular Testing Guideline for Selection of Lung Cancer Patients for EGFR and ALK Tyrosine Kinase Inhibitors: Guideline from the College of American Pathologists (CAP), International Association for the Study of Lung Cancer (IASLC), Association for Molecular Pathology (AMP) Arch Pathol Lab Med. 2013 Jun;137(6):828-860.
- Pirker R, Herth FJ, Kerr KM, et al. European EGFR Workshop Group. Consensus for EGFR mutation testing in non-small cell lung cancer: results from a European workshop. J Thorac Oncol. 2010; Oct;5(10):1706-1713.
- Thunnissen E, Beasley MB, Borczuk AC, et al. Reproducibility of histopathological subtypes and invasion in pulmonary adenocarcinoma. An international interobserver study. Mod Pathol. 2012; Dec;25(12):1574-1583.
- Travis WD, Brambilla E, Müller-Hermelink HK et al, eds: World Health Organization Classification of Tumours: Pathology and Genetics of Tumours of the Lung, Pleura, Thymus and Heart. Lyon, France: IARC Press; 2004.
- Travis WD, Brambilla E, Noguchi M, et al. International association for the study of lung cancer/American thoracic society/European respiratory society international multidisciplinary classification of lung adenocarcinoma. J Thorac Oncol. 2011; Feb;6(2):244-285.
- Yoshizawa A, Motoi N, Riely GJ, et al. Impact of proposed IASLC/ATS/ERS classification of lung adenocarcinoma: prognostic subgroups and implications for further revision of staging based on analysis of 514 stage I cases. Mod Pathol. 2011; May,24(5):653-664.
Author
2013
Mary Beth Beasley, MD
Surgical Pathology Committee
Mt. Sinai Medical Center
New York, NY
Answer Key
- Minimally invasive adenocarcinoma (e).
- Adenocarcinoma, predominantly micropapillary type (c).
- Evaluation for ALK mutations should be performed by FISH analysis (d).