Clinical Summary
A 4-year-old boy is brought by his parents to see his pediatrician because they notice that his abdomen is distended. Two years ago, he underwent a partial hepatic resection for malignancy. One year after surgery he developed pulmonary metastasis. In the office, the pediatrician performs a thorough examination and orders imaging, which identifies multiple hepatic nodules confined to one lobe. The boy receives chemotherapy and undergoes another hepatic resection. The submitted slides are from the current hepatic resection.
Master List of Diagnoses
- Embryonal sarcoma
- Focal nodular hyperplasia
- Hepatoblastoma
- Hepatocellular carcinoma
- Mesenchymal hamartoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2016, case 13, and is a hepatoblastoma.
Criteria for Diagnosis and Comments
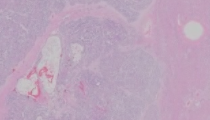
Sections demonstrate a non-cirrhotic liver with multiple nodules composed of polygonal cells with indistinct cell borders. These cells are arranged in trabeculae, nests, sheets, and cords depending on the slide evaluated. The trabeculae appear thickened with many areas being over 6 cells thick. The cytoplasm of these cells varies from eosinophilic and granular to clear. The nuclei are somewhat vesicular in nature with some having irregular nuclear contours while other areas are more round-to-oval in nature. Nucleoli are easily identified in some areas, while in other areas they are not as prominent. Mitotic activity is identified with some areas having 2 mitoses per high power field. Thin-walled vascular channels with associated red blood cells are easily identified. There are large areas of necrosis with associated microcalcifications in some slides. No heterologous elements, intratumoral bile ducts, or marked pleomorphism is present.
Hepatoblastoma (HB) is the most common liver tumor in children, accounting for two-thirds of all primary malignant liver tumors; however, it is still extremely rare (overall incidence of 1.5 cases per million). It most frequently involves children under the age of 5, with most tumors occurring in the first two years of life (mean age of diagnosis being 19 months). There is a slight male predominance. While the underlying etiology is not known, prematurity and low birth weight are strongly associated with HB. Children most commonly present with abdominal enlargement, many times with accompanying weight loss or anorexia. Thrombocytosis, anemia, and elevated alpha fetal protein (AFP) levels are found in many patients, but not all. The overall incidence of HB has increased over the last few decades; however, it is unclear if this is due to advances in imaging or early detection.
HB most commonly involves the right lobe of liver and is usually solitary, but multifocality can occur. HB is usually well-circumscribed and can measure up to 25.0 cm in diameter. HB commonly has a lobulated appearance on cut section that can vary in color depending on the differentiation of the tumor and the presence or absence of a mesenchymal component. A pseudocapsule can sometimes be present. Areas of hemorrhage and necrosis may be present (as in this case) and may predominate after chemotherapy. Ossification and calcification can also occur.
Congenital abnormalities occur with low frequency in HB. The genitourinary tract seems to be the most common site and some abnormalities described include horseshoe kidney, kidney dysplasia, and duplicated ureter. HB is known to be associated with multiple conditions including Beckwith-Weidman syndrome and familial adenomatous polyposis coli (FAP) along with some more esoteric entities.
HB morphologically mimics fetal and embryonal cells at various stages of normal liver development. In the most recent World Health Organization (WHO) Classification of Tumours of the Digestive System, HB is histologically classified into wholly epithelial type, mixed epithelial and mesenchymal type, or not otherwise specified (NOS). These histologic classifications are further subtyped and display distinct histologic patterns that can vary in amount.
Wholly epithelial HB is subtyped into fetal, mixed fetal and embryonal, macrotrabecular, and small cell undifferentiated (SCUD). The most common of all wholly epithelial subtypes is fetal which accounts for one third of all HB cases. These tumors are composed of trabeculae of small-to-medium sized polygonal cells that resemble hepatocytes in the developing liver. Their cytoplasm can vary with some cells having granular abundantly eosinophilic cytoplasm, while others are amphophilic or clear in nature. This variation of cell cytoplasm can cause a varied appearance at low power. The nucleus is usually small and centrally placed with no nuclear atypia. Mitoses are usually less than 2 per 10 high-power fields for the most common fetal variant. Mixed fetal and embryonal subtype is the second most common wholly epithelial subtype. It has fetal cells similar to the purely fetal subtype; however, there is an embryonal component that resembles liver cells at 6-8 weeks gestation. These cells have scant, granular cytoplasm devoid of visible glycogen and lipid droplets. The nuclei resemble blastemal cells with coarse chromatin. The nuclei are larger than those in the fetal subtype and frequently are angulated or oval in shape. Mitoses are easily identified, and extramedullary hematopoiesis may be present. The macrotrabecular subtype is classified based on its growth pattern with trabeculae that are 6 to 12 cells or more in thickness. This subtype should only be applied to those tumors with prominence of the macrotrabecular pattern. This subtype is composed of fetal and embryonal cells along with a third larger cell type that resembles hepatocytes. This type is the most difficult to recognize because it can resemble hepatocellular carcinoma (HCC) depending on what cell type is present. The last wholly epithelial subtype is SCUD, which is composed of discohesive small cells resembling a small blue cell tumor. The current case is best classified in this wholly epithelial category. It is unknown what the original diagnosis of the prior resection was, but the current resection has features suggestive of the macrotrabecular subtype. However, definitive classification is difficult post chemotherapy.
The mixed epithelial and mesenchymal type is comprised of epithelial and mesenchymal elements, as implied by the name. It is broken up into those without teratoid features and those with teratoid features. The epithelial component usually consists of fetal or mixed fetal /embryonal elements. The mesenchymal component is histologically neoplastic. The mesenchymal component is most commonly comprised of mature and immature fibrous tissue, and osteoid and osteoid-like tissue. Occasionally hyaline cartilage is identified. All those HBs that do not fit in the above classifications are termed NOS.
The two most common molecular pathways involved in HB are Wnt/beta-catenin and the insulin growth factor. The most common mutation involves CTNNB1 (β-catenin) (approximately 70% of all sporadic HBs). Cytogenetic defects also have been described in HB with the most common abnormalities involving 1q. There does seem to be a correlation between molecular findings and the histologic types for many HBs.
Surgery and liver transplantation are two options for treating HB with liver transplantation being utilized in those patients with unresectable tumors. However, less than 40% of patients have resectable disease at the time of diagnosis due to tumor size or because the tumor involves both hepatic lobes. Chemotherapy plays a significant role no matter what surgical option is chosen. Chemotherapy has a greater than 80% success rate in decreasing the tumor size. Preoperative chemotherapy has improved the overall 5-year survival rate to 75% in resectable HBs. Resection completeness and tumor stage are significant prognostic factors. Histologic pattern, except for possibly small cell undifferentiated and those with rhabdoid features, does not independently effect survival when adjusted for other variables. The lung is the most common site of metastasis, as seen in this case.
Chemotherapy can result in secondary changes to the tumor cells which includes cell enlargement with or without ballooning, marked nuclear abnormalities, and fatty change. Post chemotherapy keratinized squamous epithelium can be found with associated foreign body giant cell reaction. Complete tumor regression can occur, unfortunately not for this patient.
The differential diagnosis includes multiple entities, either histologically and/or by imaging and clinical scenario. Embryonal sarcoma is an extremely aggressive tumor composed of undifferentiated mesenchymal cells. This tumor usually affects children, but the age group is somewhat older than our patient. Predominantly these tumors are composed of myxoid tissue with cells of various morphologies including spindle, oval, stellate, or epithelioid. These cells tend to be markedly pleomorphic and contain intra and extracellular eosinophilic hyaline globules that are PAS-positive and diastase resistant. The diagnosis of focal nodular hyperplasia does not make sense, clinically or histologically. Clinically, focal nodular hyperplasia (FNH) is a “reach” as the diagnosis because FNHs do not metastasize. In addition, FNHs histologically demonstrate fibrous septa with abnormal large arteries with eccentric thickening. The cell plates of FNH are also only 2 cells thick.
HCC is definitely in the differential diagnosis of this case. HCC is more common in the second decade of life but can occur in younger patients if chronic liver disease is present. Key factors in separating HCC from predominantly wholly epithelial HB include age at time of diagnosis and the histological pattern. The macrotrabecular subtype can be difficult to distinguish. However, in most cases, fetal, embryonal, or mesenchymal elements can be identified in the tumor. In the literature, some suggest immunohistochemistry may play a role in separating these entities; however, a thorough histologic examination looking for these primitive areas seems to be the best tool. Fibrolamellar HCC can sometimes occur in this age group. Besides the obvious differences in histology with the lamellar fibrosis and oncocytic hepatocytes being present in fibrolamellar HCC, there has been a recent finding of a recurrent translocation involving DNAJB1-PRKACA. To date this abnormality has only been found in fibrolamellar HCC. AFP levels are not useful in differentiating HCC from HB because AFP is elevated in 90% of patients with HB. Rarely, some of hepatic tumors may have features of both hepatoblastoma and HCC. These tumors are termed transitional liver cell tumors.
Mesenchymal hamartoma will enter into the differential diagnosis due to the patient’s age. However, the clinical scenario of recurrence and metastasis does not fit. In addition, histologically these lesions are composed of loose connective tissue, bile ducts and hepatic parenchyma in a disorganized pattern.
As in most things in life, everything is not always clear cut.
Supplementary Questions
- Which gene is most commonly mutated in hepatoblastoma?
- BRAF
- CTNNB1 (β-catenin)
- DNAJB1-PRKACA
- KRAS
- SMAD4
- At which of the following ages would the diagnosis of hepatoblastoma most likely be made?
- 2 years of age
- 6 years of age
- 14 years of age
- 32 years of age
- 38 years of age
- Which of the following is not a subtype of wholly epithelial type hepatoblastoma?
- Fetal
- Giant cell
- Macrotrabecular
- Mixed fetal and embryonal
- Small cell undifferentiated
References
- Ayllon TD, Gómez BO, Ciria-Bru R, et al. Efficacy of neoadjuvant therapy and surgical rescue for locally advanced hepatoblastomas: 10 year single-center experience and literature review. World J Gastroenterol. 2014; 7;20(29):10137-10143.
- Bosman, F, Carneiro F, Hruban R, Theise N. World Health Organization Classification of Tumours of Digestive System. Lyon, FR: IARC;2010.
- Burt A, Portmann B, Ferrell L eds. MacSween's Pathology of the Liver, 6th Edition: Expert Consult. London, UK: Churchill Livingstone Elsevier; 2012.
- Ferrell L, Kakar S. Liver Pathology (Consultant Pathology). New York, NY: demosMedical; 2011.
- Graham RP, Jin L, Knutson DL, et al. DNAJB1-PRKACA is specific for fibrolamellar carcinoma. Mod Pathol. 2015;28(6):822-829.
- Mokkapati S, Niopek K, Huang L, et al. β-catenin activation in a novel liver progenitor cell type is sufficient to cause hepatocellular carcinoma and hepatoblastoma. Cancer Res. 2014;74(16):4515-4525.
- Venkatramani R, Spector LG, Georgieff M, et al. Congenital abnormalities and hepatoblastoma: a report from the Children's Oncology Group (COG) and the Utah Population Database (UPDB). Am J Med Genet A. 2014;164A(9):2250-2255.
Author
2016
William V. Chopp, MD FCAP
Surgical Pathology Committee
Michigan Pathology Specialists
Grand Rapids, MI
Answer Key
- CTNNB1 (β-catenin) (b)
- 2 years of age (a)
- Giant cell (b)