Clinical Summary
A 24-year-old woman with no significant medical history presents with vague persistent abdominal discomfort. On computed tomography (CT) imaging a 5.3 cm, solitary, well-circumscribed liver lesion with a central area of scarring is identified within the left hepatic lobe. A resection of the lesion is performed.
Master List
- Fibrolamellar hepatocellular carcinoma
- Focal nodular hyperplasia
- Hepatic adenoma
- Hypervascular metastasis
- Regenerative nodule
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2015, case 15, and is focal nodular hyperplasia.
Criteria for Diagnosis and Comments
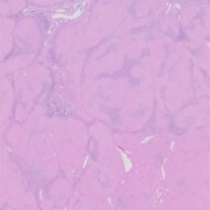
Sectioning of the specimen reveals a well demarcated but non-encapsulated light brown 5.3 cm mass that bulges from the surrounding liver parenchyma. Centrally, the lesion contains a white-gray area of stellate scarring that radiates to the periphery of the lesion. The lesion consists of nodular areas of well differentiated hepatocytes arranged in plates of no more than 2 cells thick. The nodules are divided by fibrous septae that contain marked bile ductular proliferation. Within the lesion, portal tract-like structures (often lacking a portal vein) are present in addition to unassociated large malformed arteries. The area of central scarring contains thickened tortuous vessels. No atypia or mitotic figures are present. These findings, as well as the radiologic imaging, are diagnostic for focal nodular hyperplasia (FNH).
Classical FNH is characterized by the presence of three histopathologic findings: abnormal nodular architecture, abnormal vasculature, and bile duct proliferation. The area of central scarring and nodular architecture can be absent in some cases (atypical FNH) variants, and mild hepatocyte atypia can be present. There is no longer a telangiectactic variant of FNH, as this has been reclassified as an inflammatory hepatic adenoma. However, marked congestion can be noted in some cases of FNH.
FNH is a non-neoplastic hyperplastic process that occurs around a site of abnormal vasculature in the liver. FNH is the second most common benign liver tumor after hemangioma. In children, it is the third most common benign liver tumor, after hemangioma and hamartoma. The prevalence of FNH has been reported to be between 0.4-3% in the adult population, accounting for approximately 8% of all primary liver tumors in adults. In children FNH accounts for only 2% of primary liver tumors. FNH occurs in both adults and children and across all demographics; however it is more common in adult females. The female to male ratio has been most commonly reported as 2:1.
FNH is most commonly asymptomatic and is encountered as an incidental finding in patients undergoing imaging for unrelated conditions. Symptoms associated with FNH can occur but are relatively infrequent. These include elevated hepatic enzymes, palpable abdominal mass, abdominal discomfort, anorexia, and fever. FNH usually occurs as a solitary lesion located in the right lobe of the liver. Less frequently, patients present with multiple lesions. Lesions usually are stable in size or decrease in size over time. However, there have been reports of FNH increasing in size secondary to oral contraceptive use or pregnancy. Due to the incidental nature of these lesions, imaging is an important component in diagnosis. They are often first identified by ultrasound, which can ultimately be limited in the ability to distinguish FNH from other lesions. CT can be useful in diagnosis, but since FNH is predominately found in women of child-bearing age MRI is often preferred.
The benign nature of FNH makes conservative treatment the best approach for this lesion. Ideally this lesion would be diagnosed by radiologic means alone with follow up studies done at three and six months. If the lesion appears consistent with FNH, it remains stable on imaging, and the patient is asymptomatic then no other follow up is required. If radiology is not definitive and the lesion appears suspicious, a biopsy can be performed to confirm the diagnosis. Rarely, resection of FNH is necessary. Some cases do become symptomatic and require intervention. Additionally, FNH can appear suspicious and cannot be definitively diagnosed by radiology alone. In these instances therapeutic resections can be done.
It is currently accepted that FNH is a hyperplastic reaction due to anomalous blood flow. Arterial malformations result in focal change in perfusion, causing hyperplasia of the surrounding liver parenchyma. This hyperplastic response is still under normal growth control, and consists of polyclonal hepatocyte proliferations. The regenerative nature of this lesion and its relation to anomalous vasculature is supported by the increased incidence of FNH in patients with Osler-Weber-Rendu disease, alongside hepatic hemangiomas, and in association with other vascular abnormalities such as varices. Molecular studies of FNH reveal activation of beta-catenin pathway, potentially a driving force for regeneration of hepatocytes. FNH has also been reported to demonstrate increased angiopoeitin-1: angiopoeitin-2 expression. Of note, the use of oral contraceptives is not related to the etiology of FNH but at some level FNH seems to be responsive to estrogen as patients on OCPs tend to have more vascular tumors and more symptoms.
The most challenging differential diagnosis for FNH is hepatic adenoma (HA). It is an important distinction to make because HA carries a risk for hemorrhage, as well a small possibility of malignant transformation. These occur in a similar patient demographic to FNH, with women of reproductive age most commonly affected, but can reaches sizes much greater than FNH. HA is composed of well-differentiated appearing monotonous hepatocytes arranged in plates of usually one or two cells thick with normal reticulin structure. No central stellate scar is present. HA lacks normal portal venous structures and the vascular structures consist only of sinusoids and arteries scattered throughout the lesion, which creates a risk for life threatening hemorrhage. Importantly, unlike FNH, HA is directly correlated to the use of oral contraceptives or use of other exogenous hormones. Due to these differences FNH can usually be distinguished from HA based on clinical history of oral contraceptives use, lack of central scar, lack of portal triads, central veins, bile duct proliferation, and fibrous septae.
FNH and HA overlap in occasional cases and recent information provides an immunohistochemical approach that resolves this problem. The overlap occurs between inflammatory adenoma and FNH. Immunohistochemistry for glutamine synthetase demonstrates a distinctive “map like” staining pattern in FNH whereas adenomas typically display other patterns of staining. In addition, most inflammatory adenomas stain with serum amyloid associated protein whereas FNH stains in only a small number of cases. Unfortunately, this strategy identifies rare overlap cases.
FNH can be distinguished from regenerative nodules by clinical history and presentation. Regenerative nodules occur in the background of cirrhosis or diffuse liver disease that would be evident clinically or by radiology at the time of presentation. In relatively young females presenting with a solitary nodule a lack of diffuse liver disease or abnormal liver function tests would help exclude regenerative nodule as a possibility.
Malignancy, including fibrolamellar hepatocellular carcinoma (FHCC) or hypervascular metastases may be possible differentials in those patients with equivocal imaging. FHCC occurs in a similar demographic population as FNH and appears similar grossly with fibrosis and central stellate scar. However, it presents with a much larger average size than FNH. FHCC consists of oncocytic well differentiated hepatocytes arranged in thickened plates, with fibrous bands, but lacks proliferative ducts and inflammatory cells within the septae, and will have atypia and necrosis not seen in FNH. Hypervascular metastasis could be excluded by lack of clinical history of malignancy, and the absence of distinct cellular atypia.
Supplementary Questions:
- Which of the following is not characteristic of focal nodular hyperplasia?
- Central stellate scar
- Fibrous septae with bile duct proliferation and lymphocytic infiltrate
- Monoclonal population of hepatocytes
- Presence of portal tract-like structures
- Solitary hepatic lesion
- Which of the following is the most common clinical presentation for focal nodular hyperplasia?
- Abdominal pain
- Hepatic hemorrhage
- Incidental finding on abdominal imaging
- Increase in liver function tests
- Mass with rapidly increasing size
- What is the etiology of focal nodular hyperplasia?
- Environmental exposure
- Hyperplastic process due to anomalous blood flow
- Increased estrogens due to oral contraceptive use
- Regenerative process due to cirrhosis
- Viral infection
References
- Aldinger K, Ben-Menachem Y, Whalen G. Focal nodular hyperplasia of the liver associated with high-dosage estrogens. Arch Intern Med. 1977;137(3):357.
- Balabaud C, Al-Rabih WR, Chen PJ, et al. Focal Nodular Hyperplasia and Hepatocellular Adenoma around the World Viewed through the Scope of the Immunopathological Classification. Int J Hepatol. 2013;2013;268625.
- John TG, Greig JD, Crosbie JL, Miles WF, Garden OJ. Superior staging of liver tumors with laparoscopy and laparoscopic ultrasound. Ann Surg. 1994;220(6): 711–719.
- Joseph NM, Ferrell LD, Jain D, et al. Diagnostic utility and limitations of glutamine synthetase and serum amyloid-associated protein immunohistochemistry in the distinction of focal nodular hyperplasia and inflammatory hepatocellular adenoma. Mod Pathol. 2014;27(1):62-72.
- Maillette de Buy Wenniger L, Terpstra V, Beuers U. Focal nodular hyperplasia and hepatic adenoma: epidemiology and pathology. Dig Surg. 2010;27(1):24-31.
- Nakanuma Y. Non-neoplastic nodular lesions in the liver. Pathol Int. 1995;45(10):703.
- Nime F, Pickren JW, Vana J, Aronoff BL, Baker HW, Murphy GP. The histology of liver tumors in oral contraceptive users observed during a national survey by the American College of Surgeons Commission on Cancer. Cancer. 1979;44(4):1481.
- Shortell CK, Schwartz SI. Hepatic adenoma and focal nodular hyperplasia. Surg Gynecol Obstet. 1991;173(5):426.
Authors
Jessica Tracht, MD
Resident in Pathology
University of Alabama at Birmingham
New Orleans, LA
Thomas Winokur, MD
Surgical Pathology Committee
Department of Pathology
University of Alabama at Birmingham
Birmingham, AL
Answer Key
- Monoclonal population of hepatocytes (c)
- Incidental finding on abdominal imaging (c)
- Hyperplastic process due to anomalous blood flow (b)