Clinical Summary
A 74-year-old man presents with crampy abdominal pain and small bowel obstruction. At surgery, numerous masses are identified in the distal small intestine and liver. The patient subsequently expires, and undergoes an autopsy.
Master List
- Metastatic large cell neuroendocrine carcinoma
- Metastatic mixed adenoneuroendocrine carcinoma (MANEC)
- Metastatic neuroendocrine tumor (NET)
- Metastatic small cell neuroendocrine carcinoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2015, case 08, and is a metastatic neuroendocrine tumor (NET).
Criteria for Diagnosis and Comments
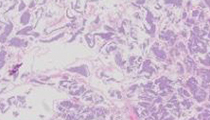
Microscopic review shows liver with a metastatic carcinoma arranged in organoid nests, composed of uniform cells with round nuclei, stippled chromatin, eosinophilic cytoplasm, and only rare mitoses (<2 mitoses per 10 high power fields). The diagnosis is a metastatic neuroendocrine tumor (NET) previously referred to as a carcinoid tumor, presumably of distal small intestinal origin.
The classification of neuroendocrine neoplasms of the digestive system has evolved to recognize and include the malignant potential of these tumors, and the classification based on grade and stage. Although the term “carcinoid tumor” was previously used for well-differentiated neuroendocrine tumors, this term implies a less aggressive tumor and frequently does not correlate with the true biologic potential of these neoplasms. All of these tumors have malignant potential, except for rare tumors in the stomach measuring less than 0.5 cm in size. Thus, in 2010, the World Health Organization (WHO) adopted the recommendations from the European Neuroendocrine Tumor Society (ENETS) to classify well-differentiated tumors of the gastrointestinal (GI) tract, liver and pancreas as neuroendocrine tumors (NETs), and high-grade small cell and large cell neuroendocrine tumors as neuroendocrine carcinomas (NECs). This system separates two broad categories of biologically distinctive neuroendocrine neoplasms, and allows for a common classification that can be utilized for tumors of all abdominal sites, regardless if the site of origin is known.
NETs are graded based on the morphologic features and the proliferative index, the latter of which includes measurement of mitotic count and Ki-67 index (% of cells with immunohistochemical [IHC] labeling for Ki-67). In general, all well-differentiated NETs are either low (G1) or intermediate grade (G2). G1 tumors have mitotic counts of <2 mitoses per 10 high power fields, and/or a Ki-67 index of <3%. G2 tumors have mitotic counts between 2 and 20 per 10 high power fields, and a Ki-67 index of 3-20%. Tumors are inherently heterogeneous, and since the determination of accurate grade is important to predict prognosis, it is recommended that at least 2,000 cells be counted (the use of image analysis is the preferred method), and areas of the tumor with the highest proliferative rates (“hot spots”) be utilized to accurately determine the grade. When mitotic counts and Ki-67 categories differ, the higher grade is utilized. Although chromogranin A and synaptophysin IHC staining may be used to confirm the histologic impression of a NET, these stains are not necessary diagnostic tools if morphologic characteristics of a NET are present. Additional IHC staining to determine peptide hormone production by NETs is in general not clinically useful, as functional NETs are defined by clinical symptoms and serum levels rather than by IHC. However, IHC stains for specific peptide hormones may be useful in some cases to correlate with a patient’s functional syndrome.
The overall incidence of NETs has increased according to Surveillance, Epidemiology, and End Results (SEER) data from 1.09 new cases per 100,000 in 1973, to 5.25 per 100,000 in 2004. This increase is most likely attributed to more sophisticated imaging and physician awareness. Gastrointestinal NETs most commonly originate in the small intestine, rectum, and the appendix. They can also occur in the colon and stomach. Small intestinal NETs equally affect males and females, often in the 6th and 7th decades of life. Gastric and appendiceal NETs are more frequently seen in females, and esophageal, ampullary, and colorectal NETs are seen more often in males. Overall, African Americans are affected more frequently than Caucasians.
Most NETs are clinically non-functional and instead present with vague nonspecific symptoms including weight loss, intermittent, crampy abdominal pain and gastrointestinal bleeding. Functional NETs present with symptoms related to hormone production such as excess production of insulin (hypoglycemia), gastrin, (peptic ulcers, diarrhea, abdominal pain, as seen with Zollinger-Ellison syndrome), vasoactive intestinal peptide (diarrhea and hypokalemia in Verner-Morrison syndrome), glucagon (hyperglycemia, diabetes mellitus and skin rash), and serotonin. Serotonin- producing tumors, almost all originating from the distal jejunum and ileum, metastatic to the liver and lymph nodes may be associated with flushing, diarrhea, and cardiac findings (such as fibrous thickening of the pulmonic and tricuspid valves), termed “carcinoid syndrome”.
NETs are generally sporadic, but a small percentage of tumors are familial. Patients with multiple endocrine neoplasia-1 (MEN-1) have an increased risk of developing functional gastrinomas, predominately in the duodenum, and rarely in the distal small bowel. Patients with von Recklinghausen disease have a risk for developing ampullary and periampullary NETs. The only factor linked to non-familial small intestinal neuroendocrine neoplasms is duodenal gastrin-producing NETs associated with Helicobacter pylori gastritis and treatment with proton pump-inhibitors.
Most small intestinal NETs already have metastatic disease at initial presentation (approximately 60% of cases), most frequently to the liver. Retrospective studies have shown that an aggressive surgical approach with resection of the primary and metastatic tumor is associated with a modest improvement in survival, and decrease of symptoms. However, the goal of surgical resection of the primary tumor and metastatic disease is only cytoreductive. Almost all patients with liver metastases who undergo resection of the metastases will have recurrent hepatic disease. Some studies have shown that resection of only the primary lesion in the presence of metastatic disease is also associated with a survival advantage. Ablative therapies such as radiofrequency ablation have been shown to be effective in decreasing symptoms and obtaining some degree of local control. Although the tumor may present as metastatic disease to the liver, determination of the primary source of liver metastases may provide helpful information for more effective, targeted chemotherapy.
The classification term neuroendocrine carcinoma (NEC) defines a poorly-differentiated high-grade malignant neoplasm. These tumors are composed of either small cells (small cell NEC) or large to intermediate cells (large cell NEC). Although they may show organoid histologic features and variable staining for synaptophysin and chromogranin, they exhibit marked cytologic atypia, frequent necrosis, and more than 20 mitoses per 10 high power fields. Due to the undifferentiated histologic appearance of large cell NECs, neuroendocrine IHC staining is necessary to confirm this diagnosis. NECs are by definition G3 tumors, defined by more than 20 mitoses per 10 high power fields, and/or a Ki-67 index of greater than 20%. In reality, most NECs have more than 50 mitoses per 10 high power fields, and Ki-67 indices of greater than 75%.
NECs of the upper small intestine are generally limited to the ampullary region where they present as nodular, ulcerated masses. They are aggressive neoplasms, composed either of small cells or large cells, both of which can resemble small and large cell neuroendocrine carcinomas of the lung. NECs of the distal jejunum and ileum have not been reported.
Mixed adenoneuroendocrine carcinoma (MANEC) is a category that includes tumors composed of both a malignant glandular component and a malignant neuroendocrine component, either of which accounts for at least 30% of the tumor. This category does not include adenocarcinomas that show focal staining for neuroendocrine IHC markers. In the upper small intestine, they are typically seen in the ampullary region, where they frequently form mucin or rarely have a squamous carcinoma component.
The extent of disease of neuroendocrine neoplasms is directly related to prognosis. For intestinal NETs, deep invasion beyond the submucosa and into or through the muscularis propria, and/or the presence of metastatic disease to regional nodes or liver is associated with a malignant course. The mortality for intestinal NETs varies depending on the site of origin, ranging from 3% (rectal), 4% (duodenal), 6% (gastric), to 21% (distal small bowel NETs). The 5 and 10 year survival rates for those NETs limited to the distal small bowel are about 72 and 60%, respectively, compared to 35 and 15% for those with liver involvement. The overall staging system used for exocrine carcinomas is not as predictive for neuroendocrine neoplasms since many of these NET patients present with stage IV disease; some patients with limited liver involvement and aggressive surgical management can experience relatively long term survival due to the characteristically slow growing nature of these tumors. Thus, a more precise staging scheme is evolving for these neoplasms. Until a formally accepted staging scheme is identified, pathologists are encouraged to use the current American Joint Committee on Cancer (AJCC) 7th edition TNM staging system which includes a common NET staging scheme for all GI NETs except for those of the pancreas and appendix (these latter two are staged in their organs’ respective TNM sections). Additional staging resources for GI NETs are the five CAP cancer protocols that have been specifically developed for GI tract NETs for each of the major anatomic sites (www.cap.org). At a minimum, pathologists should consistently record various pathologic features of these tumors, including tumor size in three dimensions, extent of bowel wall invasion, number of involved lymph nodes including size of largest metastasis, and status of resection margins of both primary tumor and resected metastatic lesions in the liver.
Supplementary Questions:
- Which of the following is true regarding neuroendocrine tumors (NETs)?
- Most NETs are associated with functioning hormone production.
- NETs show mild to moderate nuclear atypia and less than 20 mitoses per 10 high power fields.
- Synaptophysin and/or chromogranin A IHC are imperative for the diagnosis of NETs.
- The term carcinoid tumor is reliably used to define tumors with a benign clinical course.
- Well-differentiated NETs are graded as G1, G2 and G3 based on mitotic activity and or Ki-67 indices.
- Which statement best describes neuroendocrine carcinomas (NECs)?
- Carcinoid syndrome is more frequently seen in NECs.
- NECs are composed of an admixture of large and small cells.
- NECs frequently occur in the distal jejunum and ileum.
- NECs of the upper small intestine are generally limited to the ampullary region.
- These tumors are typically graded as G2 or G3.
- All of the following statements are true regarding gastrointestinal neuroendocrine neoplasms except:
- NECs are highly aggressive tumors with a poor prognosis.
- Stage IV NETs are invariably associated with a short survival.
- Surgical removal of the primary lesion(s) in conjunction with liver metastases is associated with an improved prognosis in NETs.
- The mortality associated with rectal NETs is lower than distal jejunal-ileal NETs.
- For intestinal NETs, deep invasion beyond the submucosa and into or through the muscularis propria tends to be associated with a malignant course.
References
- Bosman FT, Carniero F, Hruban RH, Theise ND, editors. WHO Classification of Tumours of the Digestive System. 4th ed. Geneva,CH: World Health Organization; 2010.
- Klimstra DS, Modlin IR, Coppola D, Lloyd RV, Suster S. The pathologic classification of neuroendocrine tumors: a review of nomenclature, grading, and staging systems. Pancreas. 2010; 39:707-712.
- Klimstra DS. Pathology reporting of neuroendocrine tumors: essential elements for accurate diagnosis, classification, and staging. Semin in Oncol. 2013;40:23-36.
- Oberg KE. The management of neuroendocrine tumours: current and future medical therapy options. Clin Oncol. 2012;24:282-293.
- Wang SC, Fidelman N, Nakakuraa EK. Management of well-differentiated gastrointestinal neuroendocrine tumors metastatic to the liver. Semin Oncol. 2013;40:69-74.
Author
Tamera J. Lillemoe, MD
Surgical Pathology Committee
Hospital Pathology Associates
Allina Health Laboratories
Minneapolis, MN
Answer Key
- NETs show mild to moderate nuclear atypia and less than 20 mitoses per 10 high power fields (b).
- NECs of the upper small intestine are generally limited to the ampullary region (d).
- Stage IV NETs are invariably associated with a short survival (b).