Clinical Summary
A 9-year-old boy is found to have abdominal distention and an abdominal mass and undergoes a right lobectomy of the liver. A 12.5 cm heterogeneous hemorrhagic, soft solid and focally cystic mass is identified in the liver. The tumor appears fairly well circumscribed, and focally is associated with rupture of the capsular surface. The tumor is located 0.3 cm from the nearest surgical margin. The surrounding hepatic parenchyma appears congested.
Master List
- Angiosarcoma
- Epithelioid gastrointestinal stromal tumor
- Hepatobiliary rhabdomyosarcoma
- Hepatoblastoma
- Undifferentiated embryonal sarcoma of liver
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2013, case 06, and is an undifferentiated embryonal sarcoma of liver.
Criteria for Diagnosis and Comments
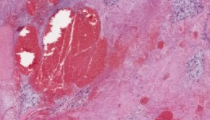
Histologically, the tumor is very cellular and is composed of a heterogeneous population of infiltrative malignant cells, with interspersed residual clusters of hepatocytes and bile ducts. The tumor cells are polymorphous with ovoid, epithelioid, and spindle shaped forms, as well as large anaplastic and multinucleated tumor cells present. Other areas show a loose, myxoid stroma with spindle and stellate tumor cells. The large anaplastic and multinucleated tumor cells have variably abundant pale pink cytoplasm and pleomorphic nuclei with coarse chromatin. Many of these large giant cells contain prominent intracytoplasmic hyaline droplets; extracellular hyaline droplets are also present. The tumor shows large areas of necrosis and cystic degeneration, associated with hemorrhage and proteinaceous fluid. These histologic features are those of an undifferentiated embryonal sarcoma of the liver (UESL).
UESL is a tumor of undifferentiated mesenchymal cells, which typically occurs in children ages 6-10, although some cases occur in older children and teenagers. Rare cases have been reported in adults up to age 73. Males and females are equally affected. Although the etiology is unknown, some cases of UESL have been reported to arise in association with mesenchymal hamartoma of liver. Patients with UESL present with abdominal pain and distention, often accompanied by weight loss and fever. These tumors grow rapidly and can be associated with hemoperitoneum and hemorrhagic shock, secondary to spontaneous tumor rupture. UESL range in size from 10.0 to 20.0 cm. On imaging these masses appear solid and variably cystic secondary to tumor necrosis and resultant cystic degeneration. On gross evaluation, the tumor is well-defined and appears gelatinous and variegated in appearance with solid gray-white tumor and interspersed areas of necrosis and hemorrhage. Microscopically, these tumors are composed of undifferentiated, polymorphous, mitotically active mesenchymal cells which exhibit stellate, oval, and spindle features with multinucleated tumor giant cells, embedded in a myxoid or fibrous stroma. Some tumor cells may be arranged in a storiform pattern simulating other sarcomas, and some small ovoid tumor cells show features suggestive of embryonal rhabdomyosarcoma or hepatoblastoma. Rare UESL cases have been reported to exhibit osteoid formation. Extramedullary hematopoiesis is present in 50% of cases.
A characteristic feature of UESL is the presence of hyaline droplets, seen within the cytoplasm of many of the large giant and anaplastic tumor cells and in the surrounding stroma. These globules are strongly PAS-positive (periodic acid-Schiff staining), diastase resistant. Electron microscopic studies reveal that these droplets are lysosomes with dense precipitates.
Immunohistochemical evaluation of UESL reveals variable staining for several markers, reflective of its probable histogenesis from primitive epithelial and mesenchymal precursors. Thus, vimentin is the only consistently positive marker seen in this tumor. Variable expression of cytokeratins, desmin, smooth muscle actin, Bcl-2, CD10, CD68, alpha-1antitrypsin, alpha-1 antichymotrypsin and calponin have been reported. No staining has been reported in UESL for HepPar-1 or alpha fetoprotein (AFP), while glypican 3 staining has been observed. Although numerous chromosomal gene rearrangements have been identified in UESL, no definitive patterns have been identified. However, some tumors have been reported to show 19q abnormalities, which have been also seen in mesenchymal hamartoma suggesting a common pathway in these tumors. The histogenesis remains unknown and despite the name, this tumor does not resemble embryonal liver cells by morphologic or immunohistochemical criteria.
Although early reports revealed very poor prognosis associated with UESL, the treatment has evolved over time. Surgery followed by various chemotherapy regimens has resulted in a marked improvement in overall survival.
The differential diagnosis of UESL includes hepatobiliary rhabdomyosarcoma and hepatoblastoma of the liver, both of which are composed of small undifferentiated cells which may share cytologic similarities with UESL. Hepatobiliary rhabdomyosarcoma occurs typically in young children, females more frequently affected than males (average age of 3 years). The mitotically active small blue cells of hepatobiliary rhabdomyosarcoma arise beneath the bile duct epithelium and may appear cytologically similar to the oval cells of UESL. However, hepatobiliary rhabdomyosarcoma will show immunohistochemical staining for MyoD1 and myogenin, both of which are not present in UESL. Similarly, hepatoblastoma also presents in young children (less than 5 years of age) and is composed of both epithelial and mesenchymal cells that can share histologic similarities with UESL. Patients with hepatoblastoma often present with serum AFP (alpha fetoprotein) elevations, which are not seen in patients with UESL. Hepatoblastoma will show immunohistochemical staining for HepPar-1 (in most subtypes) and nuclear staining for beta-catenin; these stains will not be positive in UESL.
Other liver tumors composed of spindle cells can also share histologic similarities with UESL. Angiosarcoma of the liver is usually seen in adults, but can rarely be identified in children. This tumor is composed of variably solid, papillary and cystic areas, composed of spindle cells with a high mitotic rate. In contrast to UESL, this tumor contains no hyaline globules and exhibits staining for CD31 and CD34. Epithelioid gastrointestinal stromal tumor can be composed of both spindle and epithelioid cells with eosinophilic cytoplasm and may contain cytoplasmic vacuoles. However, immunohistochemical markers characteristic for gastrointestinal stromal tumor including CD117 (Kit), CD34, and DOG1 are absent in UESL.
Supplementary Questions:
- Which of the following best describes undifferentiated embryonal sarcoma of liver?
- Multiple tumor nodules formed by small undifferentiated cells
- Primitive small tumor cells, resembling fetal liver
- Polymorphous spindle, ovoid, and anaplastic tumor cells with intracytoplasmic globules
- Tumor nodules composed of malignant spindled cells associated with cytoplasmic vacuoles
- Which entity shares 19q abnormalities with some cases of embryonal sarcoma, suggesting a possible shared pathway?
- Bile duct hamartoma
- Hepatobiliary rhabdomyosarcoma
- Hepatoblastoma
- Mesenchymal hamartoma
- Positive staining for which immunohistochemical marker(s) can be seen in UESL?
- Cytokeratin
- Desmin
- Vimentin
- All of the above
- None of the above
References
- Ferrell LD. Benign and malignant tumors of the liver. In: Odze RD, Goldblum JR, Crawford JM, eds. Surgical Pathology of the GI Tract, Liver, Biliary Tract, and Pancreas. 2nd Ed. Philadelphia, PA: Saunders; 2009:1322-1323.
- Frankel WL, Zhou X. Embryonal Sarcoma. In Ferrell LD, Kakar S, eds. Liver Pathology. 1st Ed. New York, NY: Demos Medical; 2011:502-504.
- Goodman ZD, Terracciano LM. Tumours and tumour-like lesions of the liver. In: Burt AD, Portmann BC, Ferrell LD, eds. MacSween's Pathology of the Liver. 5th Ed.Philadelphia, PA: Churchill Livingstone Elsevier; 2007: 803-804.
- Kiani B, Ferrell LD, Qualman S, Frankel WL. Immunohistochemical analysis of embryonal sarcoma of the liver. Appl Immunohistochem Mol Morphol. 2006 Jun; 4(2):193-197.
- Levy M, Trivedi A, Zhang J, Miles L, Mattis AN, Kim GE, Lassman C, Anders RA, Misdraji J, Yerian LM, Xu H, Dhall D, Wang HL. Expression of glypican-3 in undifferentiated embryonal sarcoma and mesenchymal harmartoma of the liver. Hum Pathol. 2012 May;43(5):695-701.
- May LT, Wang M, Albano E, Garrington T, Dishop M, Macy ME. Undiffentiated sarcoma of the liver: a single institution experience using a uniform treatment approach. J Pediatr Hematol Oncol; 2012 Apr;34(3): 114-116.
- Miettinen M, Fletcher CDM, Kindblom LG, et al. Mesenchymal tumours of the liver. In: Bosman FT, Carneiro F, Hruban RH, Theise ND, eds. WHO Classification of Tumours of the Digestive System. 4th Ed. Lyon, France: IARC Press; 2010:246-247.
- Nicol K, Savell V, Moore J, Teot L, Spunt SL, Qualman S; Children's Oncology Group, Soft Tissue Sarcoma Committee. Distinguishing undifferentiated embryonal sarcoma of the liver from biliary tract rhabdomyosarcoma: a Children's Oncology Group study. Pediatr Dev Pathol. 2007 Mar-Apr;10(2):89-97.
- O'Sullivan MJ, Swanson PE, Knoll J, Taboada EM, Dehner LP. Undifferentiated embryonal sarcoma with unusual features arising within mesenchymal hamartoma of the liver: report of a case and review of the literature. Pediatr Dev Pathol. 2001 Sep-Oct;4(5):482-489.
- Shehata BM, Gupta NA, Katzenstein HM, Steelman CK, Wulkan ML, Gow KW, Bridge JA, Kenney BD, Thompson K, de Chadarévian JP, Abramowsky CR. Undifferentiated embryonal sarcoma of the liver is associated with mesenchymal hamartoma and multiple chromosomal abnormalities: a review of eleven cases. Pediatr Dev Pathol. 2011 Mar-Apr;14(2):111-116.
Author
2012
Rajan Dewar, MD, PhD, FCAP
Surgical Pathology Committee
Beth Israel Deaconess Hospital and Harvard Medical School
Boston, MA
Answer Key
- Polymorphous spindle, ovoid, and anaplastic tumor cells with intracytoplasmic globules (c).
- Mesenchymal hamartoma (d).
- All of the above (d).