Clinical Summary
A 50-year-old woman presents with a sudden onset of right flank pain following a 2–3 day history of low-grade fevers. She recalls having urinary tract infections in the distant past. Currently, she does not respond to antibiotic therapy. A computerized tomography (CT scan) shows an irregularly shaped right kidney with dilatation of the pelvis but no evidence of urinary tract calculi. She undergoes a right simple nephrectomy. Gross examination demonstrates a deformed 8.7 x 7.1 x 4.0 cm kidney with a coarsely granular cortical surface. Serial sections reveal blunted renal calyces with firm gray-white areas, interspersed tan-pink parenchyma, a dilated renal pelvis and proximal ureteral thickening.
Master List
- Acute interstitial nephritis with granulomas
- Chronic pyelonephritis with granulomas
- Hypertensive nephrosclerosis with granulomas
- Renal papillary necrosis with granulomas
- Xanthogranulomatous pyelonephritis
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2014, case 09 and is chronic pyelonephritis with granulomas.
Criteria for Diagnosis and Comments
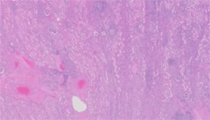
Histologic examination demonstrates patchy areas of renal parenchymal atrophy with prominent scar formation, fibrosis, areas of global glomerulosclerosis , loss of tubules and prominent interstitial inflammation. The inflammation is predominately lymphohistiocytic, which suggests a chronic inflammatory process. Well-formed granulomata are noted in this case. Some dilated renal tubules contain colloid-like proteinaceous aggregates (known as “thyroidization of renal tubules”). While the histologic findings are not entirely specific for chronic pyelonephritis, the diagnosis is rendered based on the combined clinical, gross, and microscopic findings.
Of particular interest in this case is the presence of granulomas, without a xanthomatous component (a lack of yellow lesions or masses grossly and lack of foamy histiocytes histologically), which raises the possibility of tuberculous pyelonephritis in the proper clinical context. In this case, a cytochemical stain for acid fast bacilli was performed and was negative for acid fast organisms. Sarcoidosis and drugs can also produce well-formed granulomata.
Chronic pyelonephritis can be divided into obstructive and nonobstructive types. The nonobstructive type is most commonly the result of prior conditions such as vesicoureteral reflux (VUR) and repeated urinary tract infections. VUR in children is more common in males, while in adults, it is more common in women, but can occur in men due to prostatic hypertrophy. As urine is retained, the increased pressure forces urine into the interstitium, which in turn prompts medullary injury, subsequent atrophy and fibrosis of the surrounding renal parenchyma. VUR has been implicated in cases of chronic pyelonephritis, especially in pediatric populations. It occurs in approximately 1% of children but has been found in up to 50% of children with recurrent urinary tract infections in some series. Siblings of children affected with VUR may also be at risk for similar abnormalities. In older patients, up to 20% of patients on chronic dialysis can develop chronic pyelonephritis. In some cases, there are needle-shaped cholesterol crystals and abundant granulomatous inflammation characteristic of xanthogranulomatous pyelonephritis. In such cases, urine cultures from patients with xanthogranulomatous pyelonephritis most frequently show organisms such as Escherichia coli or Proteus mirabilis.
The clinical presentation of chronic pyelonephritis depends on the etiology. Symptoms may mimic those of acute pyelonephritis, with a symptom-free period followed by acute onset of pain as the renal system is no longer able to accommodate for the increased urinary retention. Symptoms of polyuria and nocturia can occur, as renal tubular concentrating ability is lost. While the clinical presentation varies, radiographic findings usually show features of renal atrophy and dilatation of the renal pelvis, with or without an identified obstructive process. The treatment and prognosis are highly variable, based on causes, extent of renal injury, and chronicity of urinary tract obstruction. Cases of tuberculous pyelonephritis have been reported, and may be considered in the differential diagnosis when granulomas are identified, particularly in the absence of a xanthomatous component.
The differential diagnosis in this case includes renal papillary necrosis, acute interstitial nephritis, and hypertensive nephrosclerosis.
Renal papillary necrosis can arise from several etiologies, such as chronic drug use, diabetes, sickle cell disease, vasculitis, or tuberculosis. Implicated drug-related etiologies in renal papillary necrosis include acetaminophen, phenacetin, and cyclooxygenase-2 (COX2) inhibitors. In female patients, renal papillary necrosis is more likely due to analgesic use, but it is more commonly related to urinary tract obstruction in male patients. Pathologic findings include degeneration and sloughing of the medullary pyramids. The degree of distribution and necrosis can provide clues to the etiology. If there are patchy features of both early and later stages of necrosis with calcification, the differential diagnosis includes a drug-related etiology. However, if all papillae are at the same stage of acute necrosis with only rare calcifications, the differential diagnosis includes diabetic nephropathy.
Acute interstitial nephritis (AIN) is most commonly caused by side effects of certain drugs, such as antibiotics and nonsteroidal antiinflammatory drugs. Other causes include infection, transplant allograft rejection, heavy metal exposure (lead, cadmium) and autoimmune phenomena (systemic lupus erythematosus, Sjogren disease), though heavy metal exposure has also been attributed to acute tubular necrosis. Pathologic findings of AIN include interstitial edema and inflammatory infiltrates; the infiltrates vary with the time frame of disease and can consist of lymphocytes, plasma cells, macrophages, eosinophils, and/or neutrophils. The glomeruli are typically spared. If the inflammation is active, there may be evidence of concomitant tubular inflammation (tubulitis) and injury (tubular necrosis).
Hypertensive nephrosclerosis can be divided into benign and malignant types. The former is associated with mild to moderate hypertension; the latter is associated with severe hypertension. Hypertensive nephrosclerosis is more common in African-Americans. Both renal artery and systemic hypertensive causes have been implicated as causes. Pathologic findings may include small kidneys with finely-granular capsular surface and deep triangular scars. Renal cortical thinning and cyst formation may be seen. While histologic sections may show focal global glomerulosclerosis, tubular atrophy, and interstitial chronic inflammation, vascular abnormalities are apparent, which include intimal fibrosis, intimal fibroelastic thickening, smooth muscle hyperplasia, and arterial luminal narrowing. Changes of afferent arterioles and small arteries include show subendothelial eosinophilic deposits, also termed "hyaline arteriolosclerosis." Cytochemical analysis with elastin can demonstrate layering of the internal elastic lamina. Immunofluorescence studies may demonstrate immunoglobulin M (IgM) and C3 deposits within arteriolar walls.
Genetic mechanisms are being explored; some examples include coding variants in the APOL1 gene in hypertensive nephrosclerosis, as well as upregulation of the mir-21 in the progression of renal fibrosis. In malignant hypertension, vascular changes are more dramatic and include arteriolar fibrinoid necrosis and hyperplastic arteriolitis (intimal thickening with "onion skinning").
Supplementary Questions:
- Although not specific, which of the following renal conditions is more commonly associated with "thyroidization" of renal tubules?
- Acute interstitial nephritis
- Chronic pyelonephritis
- Hypertensive nephrosclerosis
- Renal papillary necrosis
- Xanthogranulomatous pyelonephritis
- Which of the following renal conditions is most commonly attributed to analgesic abuse?
- Acute interstitial nephritis
- Chronic pyelonephritis
- Hypertensive nephrosclerosis
- Renal papillary necrosis
- Xanthogranulomatous pyelonephritis
- Which of the following renal conditions is most commonly associated with hypersensitivity to an antibiotic?
- Acute interstitial nephritis
- Chronic pyelonephritis
- Hypertensive nephrosclerosis
- Renal papillary necrosis
- Xanthogranulomatous pyelonephritis
References
- Bostwick DG, Cheng L, eds. Urologic Surgical Pathology. 2nd ed. Philadelphia, PA: Mosby Elsevier; 2008:45-58.
- Brix AE. Renal papillary necrosis. Toxicol Pathol. 2002;30(6):672-674.
- Kopp JB. Rethinking hypertensive kidney disease: arterionephrosclerosis as a genetic, metabolic, and inflammatory disorder. Curr Opin Nephrol Hy. 2013;Mar10 [Epub ahead of print].
- Li L, Parwani AV. Xanthogranulomatous pyelonephritis. Arch Pathol Lab Med. 2011;135(5):671-674.
- Praga M, González E. Acute interstitial nephritis. Kidney Int. 2010;77(11):956-961.
- Zhou M, Netto G, Epstein J. Uropathology. Philadelphia, PA: Saunders Elsevier; 2012;245-263.
Authors
2014
Milon Amin, MD
Pathology Fellow
University of Pittsburgh Medical Center
Pittsburgh, PA
Alyssa M. Krasinskas, MD
Surgical Pathology Committee
Emory University School of Medicine
Atlanta, GA
Answer Key
- Chronic pyelonephritis (b). Renal papillary necrosis (d). Acute interstitial nephritis (a).