Clinical Summary
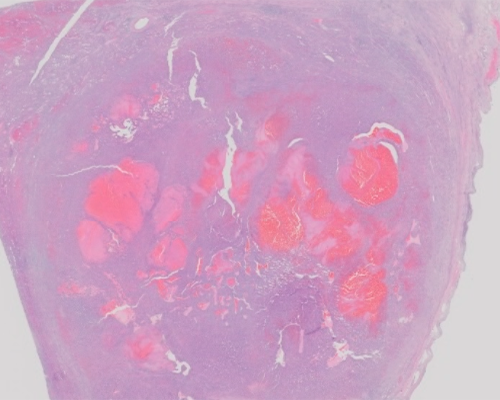
A 23-year-old woman presents with a one-year history of fatigue. Imaging studies reveal a large right atrial mass, which is resected. On gross examination, the resected mass measures 8.5 x 8.0 x 6.5 cm. The epicardial surface is covered with red-tan soft nodules and adipose tissue. The endocardial surface is white-tan to red. Sectioning reveals a fairly well-defined tumor with a mottled, firm, white-tan cut surface containing hemorrhagic and cystic areas. The mass abuts but does not grossly invade adjacent papillary muscles. Approximately 30% of the tumor is necrotic.
Master List of Diagnoses
- Angiosarcoma
- Hemangioma
- Metastatic melanoma
- Myxoma
- Synovial sarcoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2016, case 32, and is an angiosarcoma.
Criteria for Diagnosis and Comments
Histologic sections show solid areas of atypical spindle cells with hyperchromatic and pleomorphic nuclei, and irregular branching and dilated, blood-filled vascular channels lined by epithelioid cells with round nuclei and prominent nucleoli. In some areas, these lining cells form papillary tufts that project into the lumen. Some of the neoplastic cells show cytoplasmic vacuoles containing red blood cells, a helpful clue to the diagnosis. Frequent mitotic figures, including atypical forms, are present. Bizarre multi-nucleated cells, undifferentiated spindle cells in storiform and herringbone patterns, and areas of necrosis are also present. Tumor invasion into the myocardium is appreciated in some sections. Numerous lymphocytes and plasma cells are admixed with tumor cells. The overall morphologic features are consistent with a diagnosis of cardiac angiosarcoma.
Sarcomas comprise 95% of all primary cardiac malignancies; the most common type is angiosarcoma. Cardiac angiosarcoma shows male predilection and average patient age is less than 65 years. Patients present with dyspnea, chest pain, and fatigue. Due to the vagueness of these symptoms, diagnosis is often delayed until the patient has developed advanced or metastatic disease. Echocardiography is the most sensitive diagnostic modality with a detection rate of greater than 95%; angiosarcoma appears as an echogenic lobular mass, usually located in the right atrium. Magnetic resonance imaging has high soft tissue contrast and can demonstrate tumor infiltration; contrast enhancement shows vascular lakes with a sunburst appearance. Endomyocardial biopsy is not recommended for diagnosis due to low sensitivity (50%).
Cardiac angiosarcomas usually affect the right atrium, where they can extend into the right atrial chamber or invade the myocardium, tricuspid valve, or vena cava. Less common primary sites include the left atrium, right pericardium, and ventricles. Grossly, angiosarcomas are hemorrhagic with a variegated cut surface containing necrotic areas. The pericardium may be thickened or discolored if invasion occurs. Histologic patterns include irregular vessels with anastomosing channels, solid growth, and Kaposi-sarcoma like areas. Vascular channels are lined by atypical endothelial cells with tufting into the lumen. By immunohistochemistry, the neoplastic cells express vascular markers including ERG, CD31, CD34, and FLI-1. Factor VIII and von Willebrand factor may be expressed but are less-sensitive markers. Tumor cells also are positive for BNH9, a monoclonal antibody against blood group-related H and Y antigen, and Wilms Tumor-1.Cytokeratin expression is variable; however, strongly positive diffuse staining should suggest an alternative diagnosis. Of note, TP53 mutation is common in cardiac angiosarcoma.
When encountering a high-grade cardiac tumor, metastasis must be ruled out. Primary cardiac tumors usually originate in the endocardium while metastatic lesions usually involve the pericardium. Renal cell carcinoma and hepatocellular carcinoma can spread to the heart by cavoatrial extension. Up to 20% of patients with widespread non-Hodgkin lymphoma will have secondary cardiac involvement at autopsy. Metastatic melanoma may present as an intracardiac mass and spindle cell melanoma may appear histologically similar to angiosarcoma requiring immunohistochemistry to determine the diagnosis. Angiosarcoma will be positive for ERG, CD34, and CD31 and negative for S-100, Melan-A, and HMB-45.
Myxomas are the most common primary cardiac tumor, but occur much more frequently in the left atrium than the right atrium in contrast to angiosarcoma. These gelatinous tumors are attached to the endocardium with a stalk. Histologically, elongated and stellate-shaped cells are present in a myxoid matrix and form concentric rings around blood vessels.
Other cardiac sarcomas tend to be left-sided. Reports of the most common subtypes are variable, likely due to small sample size and changes in sarcoma classification over time, but include synovial sarcoma, leiomyosarcoma, and myxofibrosarcoma, all of which can histologically resemble high-grade angiosarcoma. The spindle cells of poorly differentiated synovial sarcoma also have prominent nucleoli, and necrosis may be present. However, tumor cells are positive for bcl-2, cytokeratin, and epithelial membrane antigen, the latter two of which confirm an epithelial component. Both monophasic and biphasic types have been reported in the heart. Leiomyosarcoma is composed of fascicles of spindle cells with cigar-shaped nuclei. Prominent mitotic activity and necrosis can be present. Tumor cells are positive for smooth muscle actin and desmin and negative for vascular markers. In myxofibrosarcoma, malignant cells are embedded in a myxoid stroma with prominent curvilinear vessels. Necrosis, pleomorphism, and mitotic activity vary with grade.
Hemangiomas can also occur in the heart and can be well-circumscribed or infiltrating. Histologically, they can be cavernous (composed of dilated thin-wall vessels), capillary, or mixed. These vessels are lined by benign endothelial cells. Mitoses, necrosis, solid growth pattern, and cellular pleomorphism are not seen.
Treatment of cardiac angiosarcoma is surgical resection, which has been shown to extend survival. Even in patients with metastatic disease, surgery provides palliative debulking. However, clear margins are usually not obtained due to the aggressive nature of this neoplasm. Cardiac transplant may be considered in patients with localized disease, but previous studies have been limited by small sample size. Additionally, cardiac transplantation is associated with many complications including pulmonary hemorrhage and edema. Radiotherapy may be beneficial though statistically significant survival benefit has not been reported. The role of chemotherapy is also poorly defined. No standardized treatment protocol exists due to the rarity of this tumor and advanced stage at presentation.
Cardiac angiosarcoma has a poor prognosis, with an estimated mean survival time of 14 months. Complications include congestive heart failure, pulmonary edema, tamponade, or pericardial effusion. Myocardial invasion can cause fatal arrhythmias. Tumor induced myocardial necrosis can lead to wall rupture. Venacaval or valvular obstruction leads to stenosis and systemic emboli. The lungs are the most common site of metastasis since tumor cells spread hematogenously from the right atrium. Other metastatic sites include the brain and liver.
Supplementary Questions
- Which of the following is the most common location of cardiac angiosarcoma?
- Left atrium
- Left ventricle
- Pericardium
- Right atrium
- Right ventricle
- Which of the following mutations is present in angiosarcoma?
- ALK
- BRAF V600E
- TP53
- SOX10
- Which of the following is true regarding cardiac angiosarcoma?
- Chemoradiation is associated with a longer survival benefit compared to surgical resection.
- Endomyocardial biopsy is a highly sensitive diagnostic procedure.
- Mean patient age is 70 years.
- The most common location for metastasis is the lungs.
- Tumor cells show diffuse cytokeratin expression.
References
- Acebo E. Clinicopathologic Study and DNA Analysis of 37 Cardiac Myxomas. Chest J. 2003;123(5):1379-1385.
- Bønnelykke-Behrndtz ML, Steiniche T, Damsgaard TE, et al. MelanA-negative spindle-cell associated melanoma, a distinct inflammatory phenotype correlated with dense infiltration of CD163 macrophages and loss of E-cadherin. Melanoma Res. 2015;25(2):113-118.
- Burke A., Jeudy J, Virmani R. Cardiac tumours: an update. Heart. 2008;94(1):117-123.
- Eftychiou C, Antoniades L. Cardiac hemangioma in the left ventricle and brief review of the literature. J Cardiovasc Med (Hagerstown). 2009;10(7):565-567.
- Hamidi M, Moody JS, Weigel TL, Kozak KR. Primary cardiac sarcoma. Ann Thorac Surg. 2010;90(1):176-181.
- Kim CH, Dancer JY, Coffey D, et al. Clinicopathologic study of 24 patients with primary cardiac sarcomas: a 10-year single institution experience. Hum Pathol. 2008;39:933-938.
- Kojima S, Sumiyoshi M, Suwa S, et al. Cardiac hemangioma: a report of two cases and review of the literature. Heart Vessels. 2003;18(3):153-156.
- Maraj S, Pressman GS, Figueredo VM. Primary cardiac tumors. Int J Cardiol. 2009;133(2):152-156.
- Okuno T, Matsuda K, Ueyama K, et al. Leiomyosarcoma of the pulmonary vein. Pathol Int. 2000;50(10):839-846.
- Patel SD, Peterson A, Bartczak A, et al. Primary cardiac angiosarcoma - a review. Med Sci Monit. 2014;20:103-109.
- Ramlawi B, Leja MJ, Abu Saleh WK, et al. Surgical Treatment of Primary Cardiac Sarcomas: Review of a Single-Institution Experience. Ann Thorac Surg. 2015.
- Schaffer LR, Caltharp SA, Milla SS, et al. Rare presentation of four primary pediatric cardiac tumors. Cardiovasc Pathol. 2016; 25:72-77.
- Zhang PJ, Brooks JS, Goldblum JR, et al. Primary cardiac sarcomas: a clinicopathologic analysis of a series with follow-up information in 17 patients and emphasis on long-term survival. Hum Pathol. 2008;39(9):1385-1395.
Authors
2016
Diana Murro, MD
Surgical Pathology Resident
Rush University Medical Center
Chicago, IL
Vijaya B. Reddy, MD
Surgical Pathology Committee
Rush University Medical Center
Chicago, IL
Answer Key
- Right atrium (d)
- TP53 (c)
- The most common location for metastasis is the lungs. (d)