Clinical Summary
The patient is a 66-year-old man who presents for combined heart and liver transplantation. The patient was in his usual state of good health until two years earlier, when he experienced a gradual onset of shortness of breath. Cardiac workup revealed biventricular wall thickening, wall motion irregularities, decreased ejection fraction, and congestive heart failure. A cardiac biopsy was performed, which triggered additional clinical testing and a diagnosis. He developed arrhythmias, necessitating placement of a biventricular defibrillator, followed by progressive decline in his cardiac status, eventually leading to transplantation. Hepatic workup showed only changes of congestion related to cardiac failure.
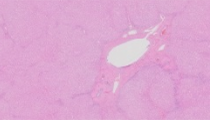
The H&E stained slide contains two portions of tissue, one from each of the explanted heart and liver.
Master List
- Amyloidosis
- Diffuse myocardial fibrosis
- Fabry disease
- Hemochromatosis
- Hypertrophic cardiomyopathy
- Sarcoidosis
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2015, case 12, and is an amyloidosis.
Criteria for Diagnosis and Comments
Histologic evaluation of the ventricular wall is remarkable for extensive interstitial, endocardial and perivascular deposits of acellular, eosinophilic extracellular matrix material, indicative of amyloid. Although specialized histochemical stains are not provided, Congo red stain highlights these deposits, and shows apple-green coloration under polarization microscopy. Sections of the liver show changes of congestive hepatopathy secondary to cardiac failure, with no evidence of amyloid deposits. The pre-transplant cardiac biopsy was diagnostic for amyloid. Further mass spectrometric and genetic testing demonstrated a hereditary pattern of amyloidosis with a mutation of the transthyretin protein.
Amyloidosis is a heterogeneous disease characterized by extracellular deposition of insoluble, misfolded protein fibrils arranged in beta-pleated sheets that may involve various organs including the heart, liver, gastrointestinal tract, nervous tissue and kidney. Amyloid accumulation may compromise blood supply and normal cell function, causing cellular atrophy, ischemia, necrosis and finally, organ failure. At least 30 different protein precursors of amyloid have been identified, manifesting as a spectrum of clinical presentations depending on type of protein and organ system involved. Amyloidosis symptoms encompass a wide phenotypic spectrum, ranging from pure sensory-motor peripheral neuropathy or autonomic dysfunction to severe heart failure. Clinically, when the heart is involved, characteristic electrocardiogram abnormalities are present in most cases and include normal to low voltage QRS amplitudes, conduction abnormalities such as atrial fibrillation or atrioventricular heart block. Two-dimensional echocardiogram findings reveal an infiltrative/restrictive cardiomyopathy and the pathognomonic feature of increased myocardial echogenicity described as a “speckled” or “sparkling” appearance of the left ventricle. Additional findings include thickening of the left ventricle and interventricular septum, biatrial dilatation and a normal to decreased ejection fraction. Cardiac MRI imaging characteristically shows transmural late gadolinium enhancement as a result of fibril deposition.
The diagnosis of amyloidosis is based on biopsy of the affected organ. A Congo red stain showing apple-green birefringence under polarization microscopy of the extracellular matrix deposits confirms the diagnosis. Rarely, electron microscopy can be utilized for diagnosis, which shows randomly arranged fibrils, 7 – 10 nm in diameter. Although the subtyping of amyloidosis on surgical pathology material can be challenging, further characterization of the specific protein involved is crucial, as the need for additional testing, prognosis and treatment vary depending on the precursor involved. Immunohistochemical assays have been utilized in many settings, but suffer from technical issues and lack of both sensitivity and specificity. Currently, laser microdissection of formalin-fixed paraffin-embedded tissue and subsequent proteomic analysis by mass spectrometry is the gold standard for classification of amyloid subtypes.
One of the most common subtypes of amyloid that infiltrates the heart is caused by transthyretin (TTR), a transport protein predominately produced by the liver, with less than 1% produced in the retina and choroid plexus. Molecular testing offers the ability to discriminate between the deposition of wild-type TTR causing senile systemic amyloidosis (SSA), versus mutated TTR causing hereditary transthyretin-related amyloidosis (ATTR). More than 100 mutations of the TTR gene have been linked to the development of ATTR. Although supportive measures to maintain fluid balance in the setting of heart failure are the mainstay of treatment of cardiac amyloidosis regardless of subtype, there is therapeutic importance in identifying the presence of a TTR mutation. In ATTR, an orthotopic liver transplant (OLT), as was performed in this case, is potentially curative and can halt the progression of disease, particularly neurologic symptoms. Transplantation can reduce plasma concentrations of the mutant TTR by more than 95% and ideally should be performed as early as possible in the disease course, preferably before cardiac involvement. Unfortunately, ATTR may still progress over time despite OLT in two settings: (1) wild-type TTR may still form amyloid fibrils in tissue where the variant TTR has already accumulated and (2) vitreous and leptomeningeal amyloidosis may progress due to continued production of extra-hepatic variant TTR. Although OLT is not indicated in cases of SSA, patients with either SSA or ATTR may benefit from cardiac transplant when severe cardiac dysfunction is present.
The differential diagnosis of cardiac amyloidosis is limited. Interstitial fibrosis as the result of processes such as ischemia, myocarditis, sarcoidosis, idiopathic or many patterns of cardiomyopathy can mimic amyloid. However, close microscopic inspection of the extracellular matrix material should highlight the collagen bundles, which are not seen in amyloid; if needed, a Congo red stain can be utilized to discern between the two. Involvement of the heart by hemochromatosis can result in scarring, which can similarly be distinguished from amyloid, as described above. Fabry disease, or alpha-galactosidase A deficiency, manifests by lysosomal accumulation of glycosphingolipids, causing a characteristic cytoplasmic vacuolization in the cardiac myocytes, which is not seen in cases of amyloid.
Supplementary Questions:
- Amyloid is characterized by all of the following, except:
- Apple-green birefringence on polarization microscopy
- Commonly involves kidneys, nerve tissue, heart, and gastrointestinal tract
- Heterogeneous disease characterized by misfolded protein fibrils 7 - 10 nm in diameter
- Only caused by native or mutated transthyretin protein
- More than 30 amyloidogenic proteins are known
- Which of the following is the best way to determine classification of amyloid subtype on formalin-fixed, paraffin-embedded tissue?
- Congo Red stain with polarization microscopy
- Flow cytometry of bone marrow aspirate
- Hematoxylin and eosin stain with dark field microscopy
- Immunohistochemical analysis by amyloid subtype panels
- Laser dissection with proteomic analysis by mass spectrometry
- With respect to cardiac involvement by hereditary transthyretin amyloidosis (ATTR), which of the following is false?
- Manifests as a restrictive cardiomyopathy
- Commonly shows amyloid deposits in the liver
- Is associated with more than 100 mutations of the transthyretin gene
- Liver transplantation reduces circulating mutated protein levels by 95%
- Some patients will benefit from heart transplantation
References
- Coelho T, Adams D, Silva A, Lozeron P, et al. Safety and efficacy of RNAi therapy for transthyretin amyloidosis. N Engl J Med. 2013;369(9):819-829.
- Dungu JN, Anderson LJ, Whelan CJ, Hawkins PN. Cardiac transthyretin amyloidosis. Heart. 2012;98:1546-1554.
- Eriksson M, Büttner J, Todorov T, et al. Prevalence of germline mutations in the TTR gene in a consecutive series of surgical pathology specimens with ATTR amyloid. Am J Surg Pathol. 2009;33(1);58-65.
- Kebbel A, Röcken C. Immunohistochemical classification of amyloid in surgical pathology revisited. Am J Surg Pathol. 2006;30(6):673-683.
- Merlini G, Vittorio B. Molecular mechanisms of amyloidosis. N Engl J Med. 2003;7:349(6):583-596.
- Mohty D, Damy T, Cosnay P, et al. Cardiac amyloidosis: Updates in diagnosis and management. Arch of Cardiovasc Dis. 2013;106:528-540.
- Rajkumar SV, Gertez MA. Advances in treatment of amyloidosis. N Engl J Med. 2007; 7:356(23):2413-2415.
- Rapezzi C, Quarta CC, Riva L, et al. Transthyretin-related amyloidoses and the heart: a clinical overview. Nature Reviews Cardiology. 2010;7:398-408.
- Sack FU, Kristen A, Goldschmidt H, et al. Treatment options for severe cardiac amyloidosis: heart transplantation combined with chemotherapy and stem cell transplantation for patients with AL-amyloidosis and heart and liver transplantation for patients with ATTR-amyloidosis. Eur J Cardio-Thorac. 2008;33(2):257-262.
- Satoskar AA, Efebera Y, Hasan A, et al. Strong transthyretin immunostaining: potential pitfall in cardiac amyloid typing. Am J Surg Pathol. 2011;35(11):1685-1690.
- Shah KB, Inoue Y, Mehra MR. Amyloidosis and the heart - A comprehensive review. Arch Intern Med. 2006;166:1805-1813.
- Speranza VD. Histologic preparations: common problems and their solutions. College of American Pathologists Press; 2009:133-137.
- Suhr OB, Herlenius G, Friman S, Ericzon BG. Liver transplantation for hereditary transthyretin amyloidosis. Liver Transpl. 2000; 6(3):263-276.
Authors
Susan J. Parson, MD, MS
Pathology Resident
Cedars-Sinai Medical Center
Los Angeles, CA
Daniel J. Luthringer, MD
Surgical Pathology Committee
Cedars-Sinai Medical Center
Los Angeles, CA
Answer Key
- Only caused by native or mutated transthyretin protein (d)
- Laser dissection with proteomic analysis by mass spectrometry (e)
- Commonly shows amyloid deposits in the liver (b)