Clinical Summary
An 18-year-old woman presents with a non-tender mass in the left breast. Breast ultrasound shows a 4.0 cm hypoechoic, oval, circumscribed mass at 4 o’clock. The mass was first noted five years prior and is stable in size. Gross examination of the excised mass reveals a well-circumscribed lesion with a tan-yellow, vaguely lobulated cut surface.
Master List of Diagnoses
- Adenomyoepithelioma
- Complex fibroadenoma
- Ductal adenoma
- Lactating adenoma
- Microglandular adenosis
- Nipple adenoma
- Nodular adenosis
- Tubular adenoma
- Tubular carcinoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2016, case 34, and is a tubular adenoma.
Criteria for Diagnosis and Comments
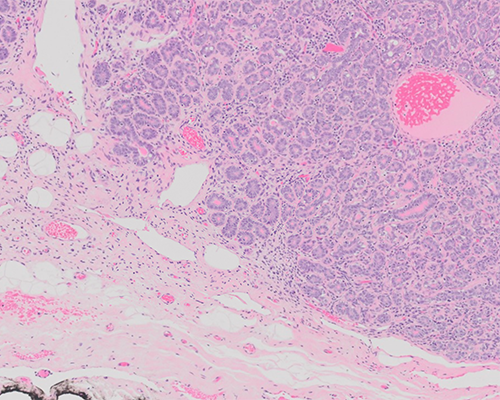
The slides show a well-circumscribed proliferation of closely packed tubular structures of uniform size lined by a single layer of epithelial cells with an often-attenuated layer of myoepithelial cells. The epithelial cells have eosinophilic cytoplasm and nucleoli are visible; however, no significant nuclear pleomorphism is present. Some tubular lumens contain brightly eosinophilic material. There is very little intervening stroma, which contains a lymphocytic infiltrate in some regions. The overall findings are characteristic of a tubular adenoma.
Tubular adenomas of the breast are uncommon benign lesions that occur in young women. They typically present as a painless, palpable nodule, and have histologic features as described above. Many of the tubular lumens appear empty; however, the eosinophilic material occasionally present has been reported to be PAS-positive, while immunohistochemically negative for α-lactalbumin. Tubular adenoma has been classified as a fibroepithelial lesion of the breast and considered by some to be a variant of the pericanalicular fibroadenoma, with an exceptionally prominent adenosis-like epithelial proliferation. Interestingly, in the current case, there appears to be an underlying intracanalicular pattern, with elongated, compressed glandular spaces. On gross examination, these lesions are reportedly softer than the average fibroadenoma, and more tan than white. Another described fibroadenoma variant, termed “complex fibroadenoma” is defined by the presence of cysts greater than 3 mm in diameter, sclerosing adenosis, papillary apocrine metaplasia, or epithelial microcalcifications. These histologic features are not a conspicuous component of the presented case.
When completely excised, tubular adenomas typically do not recur. Although rare cases of carcinoma involving these tumors have been reported, this is thought to be a coincidental association. Tubular adenomas may be distinguished histologically, and sometimes clinically, from a number of other benign, mass-producing breast proliferations, as discussed below.
Lactating adenomas, also termed nodular lactational hyperplasia, occur almost exclusively in patients who are pregnant or postpartum. While these lesions are also relatively well-circumscribed and comprised of a compact aggregate of lobules, lactating adenomas may be distinguished by the presence of lactational change with abundant cytoplasmic vacuolization. Immunohistochemistry is not usually necessary for diagnosis; however, α-lactalbumin is present in the epithelium of lactating adenomas and absent in tubular adenomas. The term nodular adenosis, or adenosis tumor, has been applied to florid sclerosing adenosis that forms a clinically identifiable mass. Microscopically, nodular adenosis consists of an aggregate of otherwise typical sclerosing adenosis, including a stromal proliferation that produces some degree of glandular compression and distortion. This contrasts with tubular adenoma, in which the glandular lumens are typically uniformly open. At low magnification nodular adenosis may appear more multinodular than tubular adenoma, given the coalescent areas of sclerosing adenosis present in the former lesion.
Tubular adenoma may also resemble the tubular variant of adenomyoepithelioma, which is a rare tumor characterized by a proliferation of layers of myoepithelial cells around epithelium-lined spaces. The epithelial cells may appear more atypical than those of tubular adenoma, given their hyperchromatic nuclei and dark staining cytoplasm. Additionally, the prominent myoepithelial cells of adenomyoepithelioma can be distinguished by their clear, glycogen-rich cytoplasm. Both lesions tend to be well-circumscribed; however, the tubular variant of adenomyoepithelioma has been reported to have a more ill-defined margin.
Although the term ductal adenoma may seem to describe the microscopic features of this case, this term actually refers to a lesion considered to be a variant of intraductal papilloma. Ductal adenoma is characterized histologically by an intraductal glandular proliferation often containing areas of apocrine metaplasia. The densely sclerotic stroma present in these lesions may compress and distort the glands leading to an infiltrative appearance; however, similar to tubular adenoma, a myoepithelial cell layer is still present around the individual glandular structures.
Unlike the described patient, those with nipple adenoma typically present with nipple discharge. Nipple adenoma is generally a well-circumscribed lesion composed of a proliferation of benign glands and ducts that retain their myoepithelial cell layer. A variety of morphologic patterns may be seen, including an adenosis-like pattern, pseudoinfiltration, and papillary or usual hyperplasia. The adenosis-like pattern might most closely resemble tubular adenoma histologically; however, similar to nodular adenosis, nipple adenoma with adenosis features displays a more sclerotic stroma with glandular distortion.
Microglandular adenosis is an uncommon mass-producing lesion of the breast that shares a few histologic features with tubular adenoma. It is similarly composed of a proliferation of rounded glands with PAS-positive intraluminal secretions. However, unlike tubular adenoma, the glands of microglandular adenosis lack an outer myoepithelial cell layer, are irregularly dispersed within fibrous stroma and adipose tissue, and contain much more prominent and uniform eosinophilic secretions. Despite its infiltrative pattern and lack of myoepithelial cells, the glands of microglandular adenosis are surrounded by basement membrane and the lesion is considered benign; however, it is often mistaken for tubular carcinoma.
Immunohistochemistry may be helpful in distinguishing these two lesions, as microglandular adenosis exhibits strong S100 expression and is EMA negative, while invasive tubular carcinoma shows the opposite staining pattern. Tubular carcinoma must also be distinguished from tubular adenoma. Despite the similar name, these two lesions appear quite dissimilar histologically, and differentiation is not usually a diagnostic challenge. Although the epithelial cells are similarly bland without significant mitotic activity, the open tubules of tubular carcinoma are often angulated and are arranged haphazardly within desmoplastic stroma, unlike the compact lobular architecture seen in tubular adenoma. Additionally, tubular carcinoma lacks myoepithelial cells, whereas even compressed myoepithelial cells in tubular adenoma can be highlighted by immunohistochemistry for markers such as p63 and smooth muscle myosin heavy chain.
Supplementary Questions
- A 22-year-old woman presents with a palpable nodule in the right breast that she noticed while breastfeeding her newborn. Which of the following is the most likely diagnosis?
- Ductal adenoma
- Lactating adenoma
- Nipple adenoma
- Tubular adenoma
- Tubular carcinoma
- A 30-year-old woman has a 1.4 cm mass excised from the left breast. Which of the following histologic features is most suggestive of a malignant diagnosis?
- Angulated tubules
- Closely approximated tubules
- Intraluminal eosinophilic material
- Open tubules
- Proliferation into adipose tissue
- Which of the following histologic features most favors a diagnosis of tubular adenoma?
- An intraductal proliferation
- Closely packed small tubules
- Lack of myoepithelial cells
- Myoepithelial cells with clear cytoplasm
- Papillary apocrine metaplasia
References
- Efared B, Sidibé IS, Abdoulaziz S, Hammas N, Chbani L, El Fatemi H. Tubular Adenoma of the Breast: A Clinicopathologic Study of a Series of 9 Cases. Clin Med Insights Pathol. 2018;11:1-5.
- Hertel BF, Zaloudek C, Kempson RL. Breast adenomas. Cancer. 1976;37:2891-2905.
- Hoda SA, Brogi E, Koerner FC, Rosen, PP. Rosen’s Breast Pathology. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2014:173-270.
- James K, Bridger J, Anthony PP. Breast tumour of pregnancy (‘lactating adenoma’). J Pathol. 1988;156:37-44.
- Lakhani SR, Ellis IO, Schnitt SJ, Tan PH, van de Vijver MJ. (eds). World Health Organization Classification of Tumours of the Breast. Lyon, FR: IARC Press; 2012;43-46,112-116.
- Schnitt SJ, Collins LC. Biopsy Interpretation of the Breast. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:153-204.
Author
2016
Rochelle A. Simon, MD
Surgical Pathology Committee
George Washington University
Washington, DC
Answer Key
- Lactating adenoma (b)
- Angulated tubules (a)
- Closely packed small tubules (b)