Clinical Summary
A 57-year-old woman presents with a breast mass. She has a history of invasive ductal carcinoma of the left breast 3 years ago, treated with partial mastectomy and postoperative radiation therapy.
Master List
- Atypical vascular lesion
- Epithelioid angiosarcoma
- Epithelioid hemangioendothelioma
- Epithelioid sarcoma
- Melanoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2013, case 20, and is an epithelioid angiosarcoma.
Criteria for Diagnosis and Comments
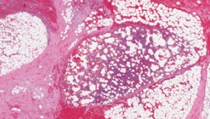
This case is an example of an epithelioid angiosarcoma of the breast secondary to radiation therapy for primary breast cancer. Angiosarcoma accounts for approximately 1 to 2% of soft tissue tumors and 0.04% of breast tumors. The most common location for traditional angiosarcoma is at cutaneous sites; however, it may be found in practically any location. Tumors in the breast may be primary or secondary to radiation. Radiation-associated angiosarcoma has been reported at other sites, including the lower abdominal wall, gastrointestinal tract, and peritoneum. Other risk factors for secondary angiosarcoma include chronic lymphedema, exposure to vinyl chloride, and foreign bodies. Angiosarcoma in general is very aggressive, with an infiltrative growth pattern, and is often multifocal at presentation. The overall prognosis is poor.
Secondary angiosarcoma is more common in postmenopausal women, whereas primary angiosarcoma is more common in premenopausal women. Most radiation-associated cases present with a painless mass within the breast parenchyma, with or without discoloration of the skin. Skin changes may include red patches, plaques, or nodules, and edema, and may resemble a hematoma. The median latency period after radiation is 5-6 years, which is shorter than post-radiation latency for angiosarcoma at other sites. At presentation, tumors are often large, extensively infiltrative and difficult to excise, commonly resulting in local recurrence. Metastatic disease at presentation is rare, but may be seen in the setting of local recurrences. As with sporadic angiosarcoma, prognosis is poor and depends on the degree of differentiation of the tumor.
On gross examination, tumors appear hemorrhagic and spongy. Within a single tumor the morphology can vary. Well differentiated tumors appear as infiltrative anastomosing vascular channels. The nuclei may be bland or show enlargement, hyperchromasia, pleomorphism, prominent nucleoli, mitotic figures, and multilayering. Intraluminal papillary structures may also be seen, which represent endothelium surrounding entrapped collagen. Other possible morphologies include poorly differentiated, epithelioid, and spindle cell patterns. Immunohistochemical staining for CD31 highlights endothelial cells and may be used to confirm the vascular origin of angiosarcoma. CD34 and factor VIII are also often positive in well and moderately differentiated tumors but may be lost in high-grade areas.
Epithelioid angiosarcoma is most common in the deep soft tissues of the extremities, but may be found almost anywhere. It is composed of large cells with large nuclei and prominent nucleoli and with abundant eosinophilic cytoplasm. It retains positivity for CD31, but is more likely than other subtypes to be cytokeratin positive. The tumor may be composed of varying proportions of epithelioid sheets and vasoformative areas and is more difficult to identify by H&E alone, especially if there are sheets of epithelioid cells.
The differential diagnosis for angiosarcoma is wide. One lesion that may be confused with well differentiated angiosarcoma in the breast, especially on biopsy, is an atypical vascular lesion. These lesions are also secondary to radiation. They appear as flesh-colored papules or red patches and are generally less than 2.0 cm. in diameter. The lesions are well circumscribed and superficial. Microscopic examination shows a proliferation of dilated, thin-walled anastomosing channels present in the superficial and mid dermis, with rare extension into the subcutaneous tissue. The channels are lined by endothelial cells that may show some atypia. In most cases, atypical vascular lesions are benign. However, there have been numerous reports of cases that have progressed to angiosarcoma. Well-differentiated, peripheral areas of angiosarcoma may be very similar in appearance to an atypical vascular lesion on biopsy, but size and superficial location can be helpful in distinguishing the two.
In angiosarcoma cases where the epithelioid component predominates, primary or metastatic carcinoma would fall into the differential diagnosis. Intracytoplasmic lumina in the endothelial tumor cells may look similar to signet ring cells, but carcinoma will not stain for the endothelial markers. It is important to remember that epithelioid angiosarcoma may show staining for cytokeratin. Epithelioid angiosarcoma with sheets of epithelioid cells may also appear histologically similar to melanoma, mesothelioma, or anaplastic large cell lymphoma. Immunohistochemistry should aid the differential diagnosis. These entities will not show positivity for the endothelial cell markers. Melanoma should show positivity for S-100, HMB-45, and Melan-A. Mesothelioma should show positivity for calretinin, CK5/6 and WT-1. Anaplastic large cell lymphoma should show positivity for LCA (CD45), CD3, and CD30.
Epithelioid sarcoma may have a morphology similar to epithelioid angiosarcoma and may even have focal vasoformative areas. Though a significant portion of epithelioid sarcomas will show CD34 positivity, they should be negative for factor VIII and CD31. Epithelioid hemangioendothelioma is rare in the breast, but cases have been reported. It is composed of variably cellular nests or cords of epithelioid to spindled cells within a myxoid or collagenous matrix. The cells may form primitive vascular lumina that may contain erythrocytes. Epithelioid angiosarcoma generally has greater cytologic atypia, vessel formation, and a predominantly sheeted growth pattern, allowing for differentiation.
Supplementary Questions
- Which of the following statements about angiosarcoma of the breast secondary to radiation therapy is false?
- At presentation, tumors are often large and locally aggressive.
- It is more common in premenopausal women than in postmenopausal women.
- It typically has a shorter latency period for development after radiation therapy than other sites.
- Prognosis is related to the degree of differentiation of the tumor.
- Tumors may present with cutaneous changes similar to primary angiosarcoma.
- Which of the following statements about angiosarcoma is false?
- Angiosarcoma may show well differentiated and poorly differentiated areas within the same tumor.
- Angiosarcoma should show positive staining for CD31, CD34, and Factor VIII, regardless of degree of differentiation.
- Classic angiosarcoma is characterized by infiltrative anastomosing vascular channels with varying degrees of nuclear size and pleomorphism.
- Which of the following statements about epithelioid angiosarcoma is false?
- Carcinoma should be considered in the differential diagnosis for epithelioid angiosarcoma due to the presence of sheets of epitheloid cells and signet ring cells that can mimic intracytoplasmic lumina.
- Cytokeratin staining can be used to rule out epithelioid angiosarcoma.
- Epithelioid angiosarcoma may be predominantly vascular or predominantly epithelioid in morphology.
- Staining for CD34 can be used to rule out other cellular neoplasms in the differential, including melanoma, mesothelioma, and anaplastic lymphoma.
References
- Billings SD, McKenney JK, Folpe AL, Hardacre MC, Weiss SW. Cutaneous angiosarcoma following breast-conserving surgery and radiation: an analysis of 27 cases. Am J Surg Pathol. 2004;28(6):781-788.
- Brenn T, Fletcher CD. Radiation-associated cutaneous atypical vascular lesions and angiosarcoma: clinicopathologic analysis of 42 cases. Am J Surg Pathol. 2005;29(8):983-996.
- Chen KT, Kirkegaard DD, Bocian JJ. Angiosarcoma of the breast. Cancer. 1980;46(2):368-371.
- Hart J, Madavilli S. Epithelioid angiosarcoma: a brief diagnostic review and differential diagnosis. Arch Pathol Lab Med. 2011;135(2):268-272.
- Lucas DR. Angiosarcoma, radiation-associated angiosarcoma, and atypical vascular lesion. Arch Pathol Lab Med. 2009;133(11):1804-1809.
Authors
2012
Amanda Treece, MD
Resident in Pathology
University of Alabama at Birmingham
Birmingham, Alabama
Thomas Winokur, M.D
Surgical Pathology Committee
University of Alabama at Birmingham
Birmingham, Alabama
Answer Key
- It is more common in premenopausal women than in postmenopausal women (b).
- Angiosarcoma should show positive staining for CD31, CD34, and Factor VIII, regardless of degree of differentiation (b).
- Cytokeratin staining can be used to rule out epithelioid angiosarcoma (b).