- Home
- Member Resources
- Pathology Case Challenge
- Anterior Mediastinum
Clinical Summary
A 33-year-old woman presents with cough and chest tightness for the past month. She was diagnosed with myasthenia gravis 5 months ago, but otherwise has no significant medical history. Chest x-ray demonstrates a large mass in the anterior mediastinum, which on CT is noted to measure 10.0 x 7.5 x 6.0 cm. CT-guided percutaneous biopsy is performed.
Master List
- Lymphoblastic lymphoma
- Thymic hyperplasia
- Thymoma, WHO type A
- Thymoma, WHO type AB
- Thymoma, WHO type B1
- Thymoma, WHO type B2
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2013, case 30, and is a thymoma, WHO type AB.
Criteria for Diagnosis and Comments
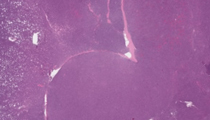
Scanning magnification shows a tumor composed of sheets of small cells separated by thin fibrous bands. On higher magnification, focal areas displaying short fascicles of spindle cells are seen, admixed with areas containing a dense lymphoid cell population. The areas displaying dense lymphoid cell population show an admixture of predominantly small lymphocytes with small spindle to oval cells showing dispersed nuclear chromatin, absence of nucleoli, and scant, indistinct rim of cytoplasm. The small lymphocytes show minimal nuclear irregularities and low mitotic activity. The small oval to spindle cell component is very similar in both the fascicular areas devoid of lymphocytes and in the lymphocyte-rich areas (so-called "B-like" component). The overall appearance is that of a biphasic tumor in which spindle cell areas completely devoid of or with few lymphocytes alternate with lymphocyte-rich areas containing fewer but similar spindle to oval cells. The findings are characteristic of type AB thymoma in the current WHO classification.
The term "thymoma" describes a collection of neoplasms that can show a wide variety of cell types and growth patterns, and exhibit variable malignant potential. These tumors are seen primarily in adult patients. They usually present as a mass in the anterior-superior mediastinum, but may occur in the neck or in other mediastinal compartments (pericardium, pleura, lung parenchyma). A high proportion of patients with thymoma (30-45%) develop myasthenia gravis (MG). These patients have historically had a worse prognosis due to myasthenic crisis, but with improvements in management, MG is no longer believed to demonstrate prognostic significance. Patients with thymomas may also be associated with a variety of other immune disorders, including hypogammaglobulinemia, myositis, dermatoyositis, myocarditis, lupus erythematosus, rheumatoid arthritis, scleroderma, Sjogren syndrome, and autoimmune enteropathy. Overall, prognosis is dependent on stage and, to a lesser degree, on histology. Surgical excision of fully encapsulated or minimally invasive thymomas is in most cases curative.
Gross appearance is usually that of a large, yellow-gray, lobulated mass. Most tumors are well-encapsulated, but 20% may show local invasion into surrounding structures. Necrosis and cystic degeneration are also common with larger tumors.
Current WHO categorization of thymomas is based on the cytologic features of the tumor cells (i.e., oval/spindle vs. round/epithelioid), degree of cytologic atypia of the epithelial cells, and relative proportion of lymphocytes to epithelial cells. The classification system utilizes a combination of numbers and letters, and includes type A, B1, B2, B3, and AB. Tumors harboring spindle/oval-shaped cells with minimal lymphocytic infiltrate are designated type A. Additional features, including microcysts, glands, and rosettes, are commonly associated with type A thymoma. Cells may be arranged in hemangiopericytic or storiform pattern, or form interlacing fascicles.
Type B thymomas, in contrast, exhibit round/plump or dendritic-appearing epithelial cells and a generally prominent lymphocytic component. Type B is further sub-categorized into B1, B2, and B3, according to the relative proportion of epithelial and lymphoid cells, and on the increase in cytologic atypia of the epithelial cells. B1 tumors are characterized by a predominance of small lymphocytes admixed with few, scattered epithelial cells. The epithelial cells have pale round vesicular nuclei with small nucleoli and are surrounded by an ample rim of cytoplasm. Pale areas of so-called "medullary differentiation" containing fewer lymphocytes, as well as distinctive cyst-like structures composed by dilated perivascular spaces are commonly present. Type B2 thymomas, while still lymphocyte-rich, contain an approximately equal admixture of epithelial cells and lymphocytes. Type B3 thymomas are characterized by a scant lymphocytic component and a predominance of round epithelial cells demonstrating cytologic atypia that frequently palisade around perivascular spaces. The nuclei are large, sometimes pleomorphic, and may adopt a raisinoid appearance, with dense chromatin and prominent nucleoli. Cytoplasm is usually abundant, and may have a pavement-like appearance due to sharp membrane demarcation.
In terms of current WHO classification, distinction of the combined type AB from pure A and B types may be a source of confusion, in light of the variable cytologic appearance of the neoplastic cells described previously. AB classification does not denote or require features of both A and B epithelial types, as the name may suggest. Rather, this diagnosis is understood to feature oval/spindle epithelial cells consistent with type A, in the context of abundant lymphocytes typically seen in type B thymomas (so-called "B-like" areas), independent of the presence or absence of epithelial cells displaying B type morphology.
Immunohistochemistry is not typically applicable to distinguishing between thymoma types, but can be quite useful in the context of differential diagnosis with other lesions. In general, thymomas of all types stain positively with cytokeratin and p63. A few novel thymic epithelial markers, including CD205 and Foxn1, have been described but are not yet widely applied in general practice. Interestingly, thymic epithelial cells, particularly of the spindle cell type, can also stain positively with CD20, a finding that is of obvious importance for differential diagnosis. The majority of lymphocytes found in thymomas are T-cells, which demonstrate immunohistochemical and enzymatic phenotypes consistent with immature thymocytes (TdT, CD99, and CD1a positive). Most thymomas, with the exception of B3, stain negative with CD5 and CD117.
Lymphoblastic lymphoma may also be part of the differential diagnosis for thymomas rich in lymphocytes. Lymphoblastic lymphomas are almost always seen in children or adolescents, although they can also present in adults and elderly patients. Presentation is often in association with blasts in peripheral blood, but may precede the leukemic phase. Histologically, lesions are characterized by medium-sized, neoplastic lymphoid cells with fine chromatin, nuclear convolutions, and inconspicuous nucleoli. Mitotic figures and necrosis are common findings. Cells are most often of T-cell lineage, and usually express immature antigens, but may exhibit antigens of mature cortical or medullary thymocytes. An easy way to separate lymphocyte-rich thymomas from lymphoblastic lymphoma is by applying immunohistochemistry with antibodies to cytokeratin; thymoma will demonstrate a fine meshwork of singly scattered keratin-positive epithelial cells admixed with the lymphoblasts, whereas lymphoblastic lymphoma will react only for T-lymphoid cell markers and will be negative for cytokeratin.
Thymic hyperplasia may also be considered in the differential diagnosis, particularly in cases of B1 type thymoma. In thymic hyperplasia, the tissue maintains a normal thymic architecture with adequately preserved cortico-medullary ratio, whereas in thymoma the normal architecture of the gland is distorted by sheets of lymphoid cells containing scattered neoplastic epithelial cells without preservation of the normal cortical/medullary architecture.
Supplementary Questions
- Which of the following best characterizes the histological appearance of type AB thymoma?
- Abundant lymphocytes resembling the normal cortex admixed with scattered round epithelial cells
- Approximately equal admixtures of lymphocytes and round epithelial cells with vesicular nuclei and mild atypia
- Atypical spindle cells admixed with equal proportions of round epithelial cells
- Neoplastic T-lymphocytes with fine chromatin, nuclear convolutions, inconspicuous nucleoli, and numerous mitotic figures and absence of epithelial cells
- Spindled, bland epithelial cells lacking atypia, admixed with lymphocytes in varying proportions, including lymphocyte-rich areas
- Which of the following stains would you expect to be negative in most thymomas?
- CD1a
- CD3
- CD5
- Cytokeratin
- p63
- Which of the following best characterizes the lymphocyte populations found in thymomas?
- Neoplastic admixed with non-neoplastic
- Neoplastic and immature
- Neoplastic and mature
- Non-neoplastic and immature
- Non-neoplastic and mature
References
- Moran CA, Weissfeldt A, Kalhor N, Solis LM, Behrens C, Wistuba II, Suster S. I. Thymomas: A clinicopathological correlation of 250 cases with emphasis on the World Health Organization (WHO) schema. Am J Clin Pathol. 2012;Mar;137(3):444-450.
- Moran CA, Walsh G, Suster S, Kaiser L. II. Thymomas: A clinicopathological correlation of 250 cases with emphasis on the World Health Organization (WHO) schema. Am J Clin Pathol. 2012;Mar; 137(3):451-481.
- Pan CC, Chen WY, Chiang H. Spindle cell and mixed spindle/lymphocytic thymomas: an integrated clinicopathological and immunohistochemical study of 81 cases. Am J Surg Pathol. 2001;Jan;25(1):111-120.
- Suster S, Moran CA. Thymoma Classification: Current status and future trends. Am J Clin Pathol. 2006;125:542-554.
- Suster S, Moran CA. Problem areas and inconsistencies in the WHO classification of thymoma. Semin Diagn Pathol. 2005;Aug;22(3):188-197.
Authors
2013
Nicholas Harding-Jackson, MD
PGY-1 Pathology Resident
Medical College of Wisconsin
Milwaukee, WI
Saul Suster, MD
Surgical Pathology Committee
Medical College of Wisconsin
Milwaukee, WI
Answer Key
- Spindled, bland epithelial cells lacking atypia, admixed with lymphocytes in varying proportions, including lymphocyte-rich areas (e).
- CD5 (c).
- Non-neoplastic and immature (d).