Clinical Summary
A 20-year-old man presents with an enlarging right testicular mass. Serum tumor marker levels are obtained prior to the radical orchiectomy with the following results: AFP, 968 ng/mL; Beta-hCG, 7 IU/L; and LDH, 236 IU/L. Gross examination of the testis reveals a single 3.0 cm somewhat circumscribed, soft, white to pale yellow mass with focal cystic degeneration, hemorrhage, and small areas of necrosis.
Master List
- Choriocarcinoma
- Embryonal carcinoma
- Juvenile granulosa cell tumor
- Seminoma
- Sertoli cell tumor
- Teratoma
- Yolk sac tumor
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2013, case 33, and is a yolk sac tumor.
Criteria for Diagnosis and Comments
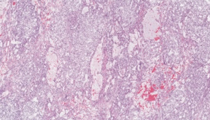
This testicular lesion is composed of sheets of round neoplastic cells with prominent cytoplasmic vacuoles ("lipoblastic-like" appearance) and thin, anastomosing cords of flat epithelial cells often forming microcysts in a myxoid background. This predominant reticular pattern is seen interspersed with macrocystic spaces containing exfoliated, degenerating tumor cells, and macrophages, along with areas of necrosis. An abundance of eosinophilic, amorphous intercellular basement membrane material is seen, as well as numerous round eosinophilic intracellular hyaline globules. These morphologic findings are characteristic of yolk sac tumor.
Yolk sac tumor occurs in both children and adults, most commonly as a pure neoplasm in children while often as a component of a mixed germ cell tumor in adults. The clinical presentation is usually a painless testicular mass and elevated serum alpha fetoprotein (AFP), often in the hundreds to thousands of nanograms per milliliter. The gross appearance varies from uniform, tan, myxoid nodules to soft, white-grey nodules with cystic degeneration, necrosis, and hemorrhage. Microscopically, yolk sac tumors exhibit many patterns:
- endodermal sinus;
- reticular (microcystic);
- papillary;
- glandular;
- solid;
- myxoid;
- macrocystic;
- polyvesicular vitelline;
- hepatoid;
- sarcomatoid;
- and parietal.
The endodermal sinus pattern is perhaps the most distinctive, characterized by the presence of "Schiller-Duval bodies" that are composed of tumor cells lining a central fibrovascular core projecting into adjacent space, resembling a glomerulus. These structures, although characteristic of yolk sac tumor, are often absent. The most common pattern, on the other hand, is the reticular pattern, which is seen as the predominant pattern in this case.
The differential diagnosis of testicular tumors includes germ cell tumors: yolk sac tumor, choriocarcinoma, embryonal carcinoma, seminoma, and teratoma; and sex cord–stromal tumors, such as juvenile granulosa cell tumor and Sertoli cell tumor. Morphologic features are usually sufficient for accurate classification of yolk sac tumor; however, immunohistochemistry may be of use when it exhibits overlapping morphology with other entities in the usual differential diagnoses. Table 1 outlines the immunoreactivity for selected testicular tumors.
Table 1. Differential immunoreactivity for testicular tumors
| OCT4 | D2-40 | EMA | AE1/AE3 | SOX2 | CD30 | GPC3 | HCG | Inhibin | |
| Seminoma | + | + | - | V | - | - | - | - | - |
| EC | + | -/+ | - | + | + | + | - | - | - |
| YST | - | - | - | + | - | - | + | - | - |
| ChorioCA | - | - | + | + | - | - | - | + | - |
| Teratoma | - | - | - | -/+ | - | - | - | - | - |
| JGCT | - | - | V | - | - | - | - | - | + |
| SCT | - | - | V | V | - | - | - | - | + |
GPC3 – glypican 3; EMA –epithelial membrane antigen; HCG –human chorionic gonadotrophin; EC – embryonal carcinoma; YST – yolk sac tumor; ChorioCA – choriocarcinoma; JGCT– juvenile granulosa cell tumor; SCT – Sertoli cell tumor; -/+ usually negative; V, variable
Seminoma is comprised of polygonal cells with prominent nucleoli, well-defined cellular borders, and clear cytoplasm, usually arranged in solid sheets with intervening fibrovascular septae containing lymphocytic infiltrates. Occasionally, yolk sac tumor can have a solid architecture with clear cytoplasm and distinct cellular borders, mimicking seminoma. It is of utmost importance to distinguish the two entities because unlike seminoma, yolk sac tumor is radioresistant. The close association with other patterns of yolk sac tumor, a higher degree of nuclear pleomorphism, intracellular hyaline globules and intercellular basement membrane material are all helpful morphologic features to correctly identify solid pattern yolk sac tumor. In more difficult cases, a concise panel of immunohistochemical stains may aid in the separation of these two entities: AE1/AE3, glypican3 (GPC3), and OCT4. The first two markers are positive in solid pattern yolk sac tumor and negative in seminoma, whereas OCT4 is positive in seminoma and negative in yolk sac tumor. A historical seminoma marker, KIT (CD117), is not helpful in distinguishing the two since a large percentage (59%) of solid yolk sac tumors also show positive reactivity with this immunostain. AFP, which is typically positive in yolk sac tumors, does not show as high of sensitivity as GPC3 in the solid pattern compared to other patterns.
Embryonal carcinoma is a common component of mixed germ cell tumor and, on gross examination, is usually irregular, grey-white, and solid with large areas of necrosis and hemorrhage. Microscopically, solid, glandular, and papillary structures can be seen. The tumor cells are irregular, pleomorphic, with prominent nucleoli, amphophilic cytoplasm, and ill-defined cytoplasmic borders; apoptosis and mitosis are readily apparent. Embryonal carcinoma may contain papillae with central blood vessels, mimicking the "Schiller-Duval bodies" of yolk sac tumor, but the papillae are lined by the typical larger embryonal carcinoma cells demonstrating a higher degree of cellular atypia, dense eosinophilic to amphophilic cytoplasm, and frequent mitosis with apoptosis. Another helpful morphologic feature is the intermingled, degenerating tumor cells, especially at the periphery of the tumor, which appear "smudged" or "applied on"; this is the so-called "applique pattern" commonly seen in embryonal carcinoma. OCT4, CD30 and GPC3 are useful in confirming the diagnosis; OCT4 and CD30 are positive while GPC3 is usually negative in embryonal carcinoma, and the staining pattern is reversed in yolk sac tumor.
Choriocarcinoma is the rarest of the germ cell tumors and is an uncommon component of mixed germ cell tumors. The gross appearance of choriocarcinoma is hemorrhagic, and this is reflected in the microscopic examination, where the hemorrhagic foci are surrounded by islands of biphasic proliferation of syncytiotrophoblast cells and cytotrophoblast cells. The sheet-like cytotrophoblastic component is capped by multinucleated syncytiotrophoblasts containing denser, eosinophilic cytoplasm. Occasionally, the presence of syncytiotrophoblast cells may be less conspicuous, and a solid proliferation of cytotrophoblasts demonstrates a "monophasic" appearance, which may simulate a solid pattern yolk sac tumor. The clinical history of a marked elevation of serum Beta-hCG level, histologic evidence of an abundance of hemorrhage with a biphasic proliferation of cyto- and syncytiotrophoblasts, along with a positive reactivity to human chorionic gonadotrophin (HCG) and epithelial membrane antigen (EMA) are diagnostic of choriocarcinoma.
Rarely, a sarcomatoid or glandular yolk sac tumor may be confused with teratoma, especially when diagnostic material is limited. Some helpful morphologic features in making the correct diagnosis include the continuity from other “classic” yolk sac tumor patterns, the lack of a circumferential smooth muscle proliferation (compared to teratoma), and the more extensive branching patterns of the glandular yolk sac tumor. The strong positive reactivity to cytokeratin and AFP or GPC3 also supports a diagnosis of yolk sac tumor over teratoma.
Juvenile granulosa cell tumor is a major differential diagnosis in infants with testicular tumors. It usually occurs in infants less than three months of age. Yolk sac tumor, however, is rare in infants less than six months old. The cystic areas of juvenile granulosa cell tumor, representing follicle-like structures, may be potentially confused for the reticular (micro- and macrocystic) patterns of yolk sac tumor. The patient's young age and lack of association with other patterns of yolk sac tumor should prompt serious consideration of juvenile granulosa cell tumor, and negative immunoreactivity for AFP along with positive reactivity to α-Inhibin confirm this diagnosis.
An uncommon differential diagnosis of testicular yolk sac tumor is Sertoli cell tumor. This tumor occurs in men of all ages, and on gross examination is usually well-circumscribed yellow-tan to white nodules; occasional cysts may be present, and hemorrhage and necrosis can be seen in malignant Sertoli cell tumors. There may be areas of solid proliferation and edema, superficially reminiscent of the micro- or macrocystic pattern of yolk sac tumor. However, cases of Sertoli cell tumors lack the presence of intratubular germ cell neoplasia (IGCNU) or the primitive cytology of yolk sac tumors. Like juvenile granulosa cell tumor, the positive reactivity with α-Inhibin is supportive of a sex cord–stromal tumor rather than a germ cell tumor.
Supplementary Questions
- Which tumor is characterized morphologically by the presence of "Schiller-Duval bodies"?
- Choriocarcinoma
- Embryonal carcinoma
- Seminoma
- Teratoma
- Yolk sac tumor
- Which of the following is not a feature of juvenile granulosa cell tumor?
- A major differential diagnosis of testicular tumors in young infants
- Negative immunoreactivity for cytokeratin
- Negative reactivity to AFP and GPC3
- Occurs most frequently in infants greater than six months of age
- Positive reactivity to α-Inhibin
- Which immunohistochemical staining pattern is typical of yolk sac tumor?
- AE1/AE3 +/–, α-Inhibin +
- CD30 +, D2-40 –, SOX2 +
- HCG +, EMA+, GPC3 –
- OCT4 –, AFP +/–, GPC3 +
- OCT4 +, D2-40 +, GPC3 –
References
- Cheng L, Sung MT, Cossu-Rocca P, et al. OCT4: Biological functions and clinical applications as a marker of germ cell neoplasia. J Pathol. 2007;211(1):1-9.
- Cheng L, Zhang S, Talerman A, et al. Morphological, immunohistochemical and fluorescence in situ hybridization (FISH) study of ovarian embryonal carcinoma with comparison to solid variant of yolk sac tumor and immature teratoma. Hum Pathol. 2010;41:716-723.
- Kao C-S, Idrees MT, Young RH, et al. Solid pattern of testicular yolk sac tumor: a morphologic and immunohistochemical study of 52 cases. Am J Surg Pathol. 2012;36:360-367.
- Ulbright TM, Emerson RE. Neoplasms of the testis. In: Bostwick DG, Cheng L, eds. Urologic Surgical Pathology. 2nd ed. Philadelphia: Elsevier/Mosby. 2008;757-862.
Authors
2013
Chia-Sui Kao, MD
Indiana University School of Medicine
Indianapolis, IN
Liang Cheng, MD
Surgical Pathology Committee
Indiana University School of Medicine
Indianapolis, IN
Answer Key
- Yolk sac tumor (e).
- Occurs most frequently in infants greater than six months of age (d).
- OCT4 –, AFP +/–, GPC3 + (d).