- Home
- Member Resources
- Pathology Case Challenge
- Soft Tissue
Clinical Summary
A 45-year-old woman presents with a mass in the left flank. The excision specimen reveals a 4.5 cm relatively well-circumscribed mass with a yellow-tan appearance.
Master List of Diagnoses
- Adult rhabdomyoma
- Alveolar soft part sarcoma
- Granular cell tumor
- Malignant granular cell tumor
- Reactive granular histiocytosis
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2016, case 37, and is a granular cell tumor.
Criteria for Diagnosis and Comments
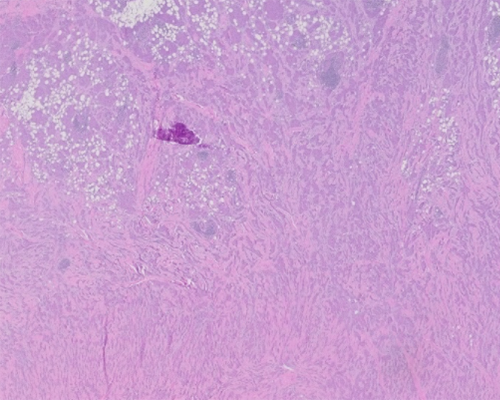
Sections show a tumor composed of nests, trabeculae, and cords of cells infiltrating skeletal muscle and adipose tissue. The tumor cells have abundant cytoplasm containing eosinophilic granules and small to intermediate size nuclei. Mitotic figures and tumor necrosis are not seen. Occasional nuclear enlargement, irregularities and hyperchromasia are noted; however, this is not a prominent feature. An immunohistochemical stain for S100 shows strong and diffuse labeling of the tumor cells. These features are consistent with a diagnosis of granular cell tumor.
Granular cell tumor (GCT) was first described by Abrikossoff in 1926 as “granular cell myoblastoma.” Subsequent observations demonstrated a histogenesis from Schwann cells and placed this entity in the family of peripheral nerve sheath tumors.
GCTs affect predominantly adults and show a 2 to 1 female to male ratio. It presents as a slow growing tumor usually less than 2 - 3 cm in diameter. GCT may affect any area of the body, most commonly involving the tongue, trunk, and limbs. Occasionally deep soft tissues, similar to current case, or internal organs may be involved. Multiple GCTs appearing synchronously or metachronously are encountered in 10% - 15% of patients. An association of GCT with Noonan and LEOPARD syndromes caused by PRPN11 gene mutations has been described.
On gross examination, GCT presents as a poorly circumscribed tumor usually less than 3.0 cm in diameter with a pale yellow-tan cut surface. Tumors involving skin or squamous mucosa are characteristically associated with prominent pseudoepitheliomatous hyperplasia, a feature mimicking squamous cell carcinoma at cursory histologic examination. The cells are arranged in sheets, trabeculae, or nests, with occasional marked desmoplastic stromal response. The lesion is not encapsulated, and the tumor cells extend along muscle fibers and nerves with apparent perineural invasion. The lesional cells are round, polygonal, or elongated with indistinct cytoplasmic borders resulting in a syncytial appearance. They have abundant cytoplasm containing characteristically numerous eosinophilic intracytoplasmic granules. Nuclei are round, centrally located, and range in size from small with condensed chromatin to large with a vesicular chromatin pattern. The cytoplasmic granules are phagolysosomes and are PAS-positive and diastase-resistant. By immunohistochemistry GCT cells express S100, neuron-specific enolase, NKI/C3, laminin, and myelin proteins and are negative for neurofilament protein and GFAP. Due to the presence of lysosomal granules, GCT is also positive for CD68. Electron microscopy shows membrane-bound autophagic vacuoles containing myelin figures and fragmented rough endoplasmic reticulum and mitochondria.
When diagnosed correctly GCTs behave in a benign fashion; local surgical excision is curative in nearly all cases.
The differential diagnosis of (benign) GCT includes malignant granular cell tumor (MGCT), adult rhabdomyoma, alveolar soft part sarcoma, and reactive granular histiocytosis.
MGCT is an exceedingly rare entity and criteria of malignancy are poorly defined. In a study by Fanburg-Smith et al, six histologic parameters have been associated with an increased risk for adverse outcome: tumor necrosis, spindling, vesicular nuclei with prominent nucleoli, > 2 mitoses/10 high power fields (200x), high nuclear to cytoplasmic ratio, and nuclear pleomorphism. To be significant, these features should be prominent in the tumor and not a focal change. The authors proposed that tumors with three or more of these features be considered malignant and those with one or two atypical. In addition, larger tumor size and advanced patient age were found to correlate with decreased survival. The current tumor demonstrates a somewhat larger size; however, it lacks the above histologic features in a significant proportion of the tumor and thus does not qualify for a diagnosis MGCT.
Adult rhabdomyoma is a rare benign skeletal muscle tumor presenting as a solitary non-tender mass in the head and neck region including pharynx, larynx, oral cavity, and tongue. It has a male predilection and median age at presentation of 60 years. The histology shows tightly packed, large, round, or polygonal cells with eosinophilic, finely granular cytoplasm resembling the histology of GCT. However, in contrast to GCT, the cells of adult rhabdomyoma demonstrate cross-striations, contain intracellular clear vacuoles caused by glycogen accumulation, and have more distinct cytoplasmic borders. In addition, rhabdomyomas lack diffuse positivity for S100, characteristic for GCT, and express muscle markers including desmin and myoglobin.
Alveolar soft part sarcoma (ASPS) is an uncommon sarcoma encountered mostly in adolescents and young adults. The tumor affects predominantly lower extremities in young adults and head and neck area in infants and children; however, other locations have also been described. Microscopic examination shows a tumor composed of polygonal cells with granular cytoplasm, distinct cell borders, large nuclei with vesicular chromatin, and prominent nucleoli. PAS-positive, diastase-resistant rhomboid or rod-shaped crystals are noted in the cytoplasm. The tumor cells form nests with central degeneration and loss of cohesion, resulting in a pseudoalveolar pattern, separated by thin-walled vascular channels. Some ASPSs demonstrate a solid or compact architecture lacking the nests and may be confused with GCT. In contrast to GCT, the cells of ASPS show more distinct cytoplasmic borders and lack diffuse and strong expression of S100 (although focal positivity may be seen). In addition, a translocation involving TFE3 and ASPSCR1 genes has been described in ASPS and can be used for diagnostic purposes.
Reactive granular histiocytosis consists of accumulations of histiocytes with granular eosinophilic cytoplasm histologically resembling GCT. It occurs usually at sites of surgical trauma or secondary to arthroplasty procedures. As opposed to GCT, the granular cells in this entity often surround nodules of granular amorphous debris and contain polarizable material.
Supplementary Questions
- Which of the following histologic features is associated with malignant granular cell tumor?
- Epithelioid morphology
- Infiltrative border
- Invasion of skeletal muscle
- Perineural invasion
- Tumor necrosis
- Which of the following immunohistochemical stains is strongly positive in granular cell tumor?
- Desmin
- HMB45
- Melan-A
- Myoglobin
- S100
- Which of the following statements best describes the granules of granular cell tumor?
- They represent intracytoplasmic accumulation of glycogen.
- They represent lysosomes.
- They represent neuroendocrine granules.
- They represent swollen mitochondria.
- They represent viral particles.
References
- Fanburg-Smith JC, Meis-Kindblom JM, Fante R, Kindblom LG. Malignant granular cell tumor of soft tissue: diagnostic criteria and clinicopathologic correlation. Am J Surg Pathol. 1998;22(7):779-794.
- Goldblum JR, Folpe AL, Weiss SW. Soft Tissue Tumors. 6th ed. Philadelphia, PA: Elsevier Saunders; 2014.
- Lack EE, Worsham GF, Callihan MD, Crawford BE, et al. Granular cell tumor: a clinicopathologic study of 110 patients. J Surg Oncol. 1980;13(4):301-316.
- McKee PH, Calonje E, Granter S. Pathology of the Skin. 4th ed. Philadelphia, PA: Elsevier Saunders; 2012.
- Miller DD, Yaar R, Posnik O, et al. Reactive granular histiocytosis secondary to arthroplasty prosthesis: a novel reaction pattern. J Cutan Pathol. 2012. 39(5):558-561.
- Moos D, Droitcourt C, Rancherevince D, Marec Berard P, Skowron F. Atypical granular cell tumor occurring in an individual with Noonan syndrome treated with growth hormone. Pediatr Dermatol. 2012;29(5):665-666.
- Tan TJ, Alassiri AH, Ng TL, Mallinson PI, Munk PL. Malignant granular cell tumor of the foot-multimodality imaging findings and literature review. Clin Imaging. 2015;39(3):543-546.
- Tsuchida T, Okada K, Itoi E, Sato T, Sato K. Intramuscular malignant granular cell tumor. Skeletal Radiol. 1997;26(2):116-121.
Authors
2016
Aleodor A. Andea, MD, MBA
Surgical Pathology Committee
University of Michigan
Ann Arbor, MI
Answer Key
- Tumor necrosis (e)
- S100 (e)
- They represent lysosomes. (b)