- Home
- Member Resources
- Pathology Case Challenge
- Placenta
Clinical Summary
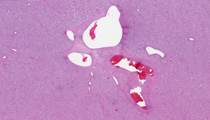
A 23-year-old G1P0 woman delivers a female neonate at 32 weeks’ gestation. The neonate has Apgar scores of 5 and 7 at one and five minutes, respectively, and is admitted to the neonatal intensive care unit due to pallor and respiratory distress. She is small for gestational age and has thrombocytopenia (platelets 80,000/mcl), but no anomalies are identified. The placenta weighs 1300 g and shows a large intraparenchymal mass measuring 10.0 cm in greatest dimension. The mass is dark red-purple on the cut surface and appears circumscribed but not encapsulated. No other lesions are identified grossly. A representative section of the placental lesion is provided.
Master List
- Angiosarcoma
- Chorangioma
- Chorangiosis
- Choriocarcinoma
- Diffuse multifocal chorangiomatosis
- Infantile hemangioma
- Localized chorangiomatosis
- Teratoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2013, case 37, and is a chorangioma.
Criteria for Diagnosis and Comments
Histologic examination of this placenta shows abrupt transition from normal vascular villi to a circumscribed monomorphous mass composed of small vascular structures. The vessels are predominantly the size of capillaries and are filled with red blood cells. Some areas show compact sheet-like arrangement of capillaries, while others show edema between the capillaries. The vascular endothelium is flat and there is no evidence of cytologic atypia. These features are typical of a chorangioma.
Chorangiomas are localized lesions of stem villi often associated with preeclampsia, multiple gestation, pregnancy at high altitudes, and late preterm birth (32-37 weeks gestation). Chorangioma was originally described by Clarke in 1798 and is the most common tumor of the placenta, with reported prevalence of approximately 1% (1 in 100 placentas). The true prevalence is unknown because many solitary minute chorangiomas can be detected only after meticulous sectioning of the placenta. It remains unclear whether chorangioma is a true neoplasm or a hamartoma-like hyperplasia of capillaries.
Chorangiomas may present as single nodules or multiple nodular masses that often project from the cut surface of the placenta, typically either subchorionic or marginal in location where there is lower oxygenation. The cut surface is firm and homogeneous and may be either red or pale tan. Histologically, chorangioma is an expansile nodular lesion composed of capillary vascular channels, intervening stromal cells and surrounding trophoblasts, and three morphologic types have been described: angiomatous (capillary), cellular, and degenerative. Angiomatous is the most common type, as in this case. The cellular variant is distinguished by increased stromal cellularity. Trophoblast hyperplasia has also been described in approximately 50% of chorangiomas, possibly as a result of excess growth factors.
Degenerative forms may show infarction, calcification, and hemosiderin deposition. Most chorangiomas are small, found incidentally, and are of no clinical significance to the mother or fetus. Intermediate-sized lesions have been associated with intrauterine-growth restriction, whereas large chorangiomas (9.0 cm or more) are associated with arteriovenous shunting and may cause polyhydramnios, hydrops fetalis, and fetal death (30-40% mortality). Fetal cardiomegaly may result from high cardiac output due to arteriovenous shunting with resultant left-to-right shunt, or chronic hypoxia due to unoxygenated blood that bypasses the maternal circulation through the vasculature of the chorangioma. Platelet sequestration in the capillaries of large chorangiomas can lead to disseminated intravascular coagulation or thrombocytopenia with associated hemorrhagic complications in the fetus.
Placental chorangiomas are most likely caused by primary dysregulation of the mesenchymal-endothelial cell interactions that determine vascular patterning within stem villi before term. Pluripotent mesenchymal stem cells, thought to reside in a paravascular location in the stem villi, may play a role in their development and, in fact, these stem cells may enter the fetal circulation and give rise to infantile hemangiomas, a clinical association described in some cases. The fact that chorangiomas occur with greater frequency in populations delivering at high altitude also lends credence to the role of reduced placental oxygenation in the pathogenesis. A genetic predisposition to chorangiomas has been suggested by increased recurrence risk in subsequent pregnancies. Unlike chorangiosis (see below), chorangiomas are not increased in diabetic pregnancies.
Two lesions related to chorangioma deserve further discussion—(1) localized chorangiomatosis and (2) diffuse multifocal chorangiomatosis. Localized chorangiomatosis is a villous stromal process with the same histologic characteristics as chorangioma, but which permeates multiple large stem villi interspersed between normal terminal villi, rather than forming a single expansile circumscribed mass. It is only occasionally detected on gross examination of the placenta. The frequency of localized chorangiomatosis is approximately 0.3% of placentas. The clinical associations and complications are similar to that described for chorangiomas.
Diffuse multifocal chorangiomatosis is defined as excessive capillary growth with surrounding pericytes and collagen, involving scattered secondary and tertiary stem villi throughout the placenta. It is quite rare with an estimated incidence of 0.2% of all placentas. Unlike localized chorangiomatosis, it is predominantly associated with very low birth weight premature infants, typically less than 32 weeks gestation. It is thought to be an aberrant response to hypoxia in immature placentas, and has been associated with pre-eclampsia, twin gestation, intrauterine growth restriction, severe congenital malformations, and placentomegaly.
The differential diagnosis of placental chorangioma and chorangiomatosis includes chorangiosis, as well as vascular neoplasms and other primary neoplasms of the placenta. Chorangiosis refers to increased numbers of capillaries (hypercapillarization) within placental villi, and represents excessive branching angiogenesis and/or folding of abnormally elongated capillaries within terminal villi. It is defined as 10 or more capillaries within 10 or more individual terminal villi in at least three areas of the placenta. It is found in approximately 7% of all placentas, predominantly term placentas, and is most commonly associated with placentas from diabetic mothers. This association is thought to be due to excessive stimulation of capillary endothelial receptors by both insulin (produced in the fetus in response to maternal hyperglycemia) and vascular endothelial growth factor A (VEGF-A),induced by intraplacental hypoxia.
Other features associated with chorangiosis include delivery at altitude, chronic villitis, fetal thrombotic vasculopathy, maternal vascular underperfusion, distal villous immaturity, and overgrowth syndromes (Beckwith-Wiedemann syndrome, Smith-Golabi-Behmel syndrome). In contrast to chorangioma, chorangiosis does not present as a gross mass lesion, but instead is a microscopic diagnosis. Localized chorangiomatosis is distinguished from chorangiosis by the presence of perivascular cells surrounding the capillaries and a background of increased stromal collagenization and cellularity, features absent in chorangiosis. Chorangioma and localized chorangiomatosis affect the mature stem villi, whereas chorangiosis affects the terminal villi, a pattern suggesting later onset of chorangiosis during placental development.
Infantile hemangioma shows morphologic similarity to chorangioma, but by definition occurs in the fetus and infant, rather than the placenta. Infantile hemangiomas have been theorized to arise from embolism of placental villi, and have been described in association with chorangiomas. Like the vasculature of the normal placenta and chorangioma, infantile hemangiomas express glucose transporter type 1 (Glut-1) by immunohistochemistry.
Angiosarcoma is a malignant neoplasm of vasculature and very rarely occurs in the placenta as a metastatic tumor. A primary angiosarcoma of the placenta has not been reported. Angiosarcoma is characterized by vascular spaces lined by endothelial cells with significant cytologic atypia and pleomorphism, and is easily distinguished from the uniform small capillaries with benign endothelium in this case.
Choriocarcinoma is a malignant neoplasm of trophoblasts which occurs very rarely as an intraplacental primary tumor and more often as a complication of gestational trophoblastic disease. It is easily distinguished from chorangioma by a proliferation of highly atypical and pleomorphic trophoblastic giant cells admixed with hemorrhage.
Teratoma is a benign germ cell tumor which occurs rarely in the placenta. Similar to other anatomic sites, teratoma of the placenta shows an admixture of mesodermal, endodermal, and ectodermal elements. The monomorphous proliferation of capillaries in chorangioma is easily distinguished from teratoma.
In summary, chorangioma is a localized neoplasm of stem villi vasculature, associated with preeclampsia, multiple gestation, and late preterm birth (32 to 37 weeks gestation). Large chorangiomas and extensive localized chorangiomatosis can be associated with polyhydramnios, hydrops fetalis, disseminated intravascular coagulation (DIC), and stillbirth. It is thought that decreased oxygen tension may play a role in the development of these vascular lesions, a hypothesis supported by the increased incidence of these entities in populations delivering at high altitude. Chorangioma may be seen in conjunction with infantile hemangiomas, and both chorangioma and localized chorangiomatosis have shown recurrence in subsequent pregnancies, suggesting an underlying predisposition in some patients.
Supplementary Questions
- Which of the following is most often associated with chorangiosis?
- Increased intervillous oxygen tension
- Infantile hemangiomas
- Maternal diabetes
- Placental mass lesion
- Prematurity
- Which of the following maternal-fetal complications may be caused by chorangioma?
- Fetal hydrops
- Gestational diabetes
- Neonatal thrombocytosis
- Oligohydramnios
- Umbilical cord thrombosis
- Which of the following lesions is characterized by a proliferation of small anastomosing capillaries surrounding secondary and tertiary stem villi, distributed throughout the placenta?
- Chorangioma
- Chorangiosis
- Diffuse multifocal chorangiomatosis
- Infantile hemangioma
- Localized chorangiomatosis
References
- Amer HZM, Heller DS. Chorangioma and related vascular lesions of the placenta – A Review. Fetal Pediatr Pathol.2010;29:199-206.
- Bagby C, Redline RW. Multifocal chorangiomatosis. Pediatr Dev Pathol. 2011 ;14:38-44.
- Benirschke K. Recent trends in chorangiomas, especially those of multiple and recurrent chorangiomas. Pediatr Dev Pathol.1999;2(3):264-269.
- Castrechini NM, Murthi P, Gude NM, E, et al. Mesenchymal stem cells in human placental chorionic villi reside in a vascular niche. Placenta.2010;31(3):203-212.
- Clark DE, Smith SK, Sharkey AM, et al. Localization of VEGF and expression of its receptors flt and KDR in human placenta throughout pregnancy. Hum Reprod.1996;11(5):1090-1098.
- FT Kraus, RW Redline, DJ Gersell, et al. Disorders of Placental Development. Placental Pathology. Fascicle 3, 1st series, Atlas of Nontumor Pathology.ARP:Washington DC;2004:61-64.
- Hiden U, Glitzner E, Hartmann M, Desoye G. Insulin and the IGF system in the human placenta of normal and diabetic pregnancies. J Anat.2009;215(1):60-68.
- North PE, Waner M, Mizeracki, et al. A unique microvascular phenotype shared by juvenile hemangiomas and human placenta. Arch Dermatol.2001;137(5):559-570.
Author
2012
Megan K. Dishop, MD
Surgical Pathology Committee
Department of Pathology, Children's Hospital Colorado
University of Colorado School of Medicine
Answer Key
- Maternal diabetes (c).
- Fetal hydrops (a).
- Diffuse multifocal chorangiomatosis (c).