- Home
- Member Resources
- Pathology Case Challenge
- Placenta
Clinical Summary
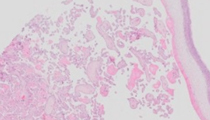
A 34-year-old G4 P3-0-0-3 presents at 27 weeks’ gestation with complaints of decreased fetal movement for 3 days, fever of 101.3°F, chills, and body aches. White blood count is 19,900/mm3 with increased neutrophils and band forms. Ultrasound examination shows fetal demise. The fetus is delivered with foul-smelling amniotic fluid, and the placenta shows a yellow-green opaque fetal surface with features suggestive of necrotizing funisitis.
Master List
- Candida albicans infection
- Escherichia coli infection
- Fusobacterium nucleatum infection
- Group B Streptococcus infection
- Listeria monocytogenes infection
- Treponema pallidum infection
- Ureaplasma urealyticum infection
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2014, case 04, and is a Fusobacterium nucleatum infection.
Criteria for Diagnosis and Comments
Histologic examination of this placenta shows an intense acute inflammatory infiltrate of the amnion and chorion, associated with extensive necrosis of the amniotic epithelium. Numerous filamentous bacterial organisms coat the surface of the partially-denuded amnion. This confluent sheet of filamentous bacilli is diagnostic of Fusobacterium spp. infection and tissue culture confirms Fusobacterium nucleatum.
Acute chorioamnionitis is the acute inflammatory response seen in the fetal membranes and umbilical cord in response to organisms in the amniotic fluid, typically bacteria. This inflammatory infiltrate is induced by the maternal inflammatory response from the intervillous space and decidua, as well as the fetal inflammatory response from the vessels of the umbilical cord and chorionic plate. Acute chorioamnionitis is suspected in a pregnant woman with fever, especially if there has been premature rupture of membranes. The incidence is higher at lower gestational ages and is associated with premature delivery. Acute chorioamnionitis is most often due to ascending infection with bacterial or mycoplasma organisms from the vaginal canal. The bacteria may be associated with bacterial vaginosis or gastrointestinal flora (group B Streptococcus, Escherichia coli, Listeria monocytogenes). The risk of neonatal sepsis is generally low, but is relatively increased for certain organisms, such as group B Streptococcus. Deleterious effects to the fetal brain white matter have been associated with the fetal inflammatory response, especially when there is umbilical arteritis in addition to phlebitis. Grossly, the placenta with acute chorioamnionitis has opaque yellow or green fetal surface and membranes. Histologic staging of chorioamnionitis based on the maternal inflammatory responses is as follows: Stage 1 (acute subchorionitis and/or acute chorionitis); Stage 2 (acute chorioamnionitis); Stage 3 (necrotizing chorioamnionitis). The fetal inflammatory response can also be classified in a similar fashion: Stage 1 (chorionic vasculitis and/or umbilical phlebitis); Stage 2 (umbilical arteritis); Stage 3 (necrotizing funisitis or concentric umbilical perivasculitis). Fusobacterium nucleatum is an anaerobic bacterial organism, which is now recognized as a relatively common cause of acute chorioamnionitis and preterm labor. Described in 1985, Fusobacterium has been generally thought to be acquired by ascending infection from fecal flora, although some now also believe that Fusobacterium nucleatum chorioamnionitis may originate from bacteria located within the oral cavity with secondary hematogenous dissemination following maternal periodontal disease. Pathologic findings associated with Fusobacterium include acute chorioamnionitis, with or without funisitis, and abundant filamentous organisms coating the surface of the amnion. Although the morphologic pattern on H&E stain is distinctive, Giemsa stain and Warthin-Starry silver stain can be used to further delineate the organism morphology. The organisms typically penetrate the amnion vertically between the amnion epithelial cells due to adherence molecules on the pointed ends.
The differential diagnosis in this case includes other causes of acute chorioamnionitis and other forms of bacterial infection in the placenta. Acute villitis and perivillositis are not typical features of Fusobacterium infection and should raise consideration of listeriosis or E. coli infection. Listeria monocytogenes is a food-borne illness, which is often acquired by maternal consumption of unpasteurized milk and cheeses, transferred hematogenously to the placenta and fetus. Listeriosis outbreaks have also been reported following consumption of deli meats, frankfurters, tacos, celery, sprouts, cantaloupe, and a variety of other contaminated foods. The histopathologic pattern associated with Listeria infection in the placenta characteristically includes acute intervillositis with intervillous microabscess formation, in addition to acute chorioamnionitis. Listeria organisms are gram-positive coccobacillary structures, but are difficult to identify on special stains. In addition to acute chorioamnionitis, E. coli and group B Streptococcus infections may result in a pattern of acute villitis due to the fetal inflammatory response in the villous capillaries during intrauterine sepsis. These bacteria do not have the filamentous appearance seen in this case. Candida infection typically results in a pattern of acute chorioamnionitis with peripheral microabscesses on the umbilical cord. This pattern has only occasionally been reported with other organisms, including Corynebacterium kutscheri, Haemophilus influenza, and Listeria monocytogenes. Although genital mycoplasma organisms (Ureaplasma urealyticum, Mycoplasma hominis) are a cause of acute chorioamnionitis, the organisms are not visible by light microscopy, in contrast to this case. Treponema pallidum infection (syphilis) typically causes a pattern of histiocyte-predominant villitis, proliferative endovasculitis, and necrotizing umbilical periphlebitis. Acute chorioamnionitis, as in this case, is not a typical feature.
Supplementary Questions:
- Which of the following causes of acute chorioamnionitis is most often associated with microabscesses in the umbilical cord?
- Candida albicans
- Escherichia coli
- Fusobacterium nucleatum
- Group B Streptococcus
- Listeria monocytogenes
- Which of the following congenital infections is suspected following maternal ingestion of unpasteurized milk?
- Candida albicans
- Fusobacterium nucleatum
- Lactobacillus
- Listeria monocytogenes
- Toxoplasmosis
- Which of the following infections may result from maternal periodontal disease?
- Escherichia coli
- Fusobacterium nucleatum
- Group B Streptococcus
- Listeria monocytogenes
- Toxoplasmosis
References
- Altshuler G, Hyde S. Fusobacteria: an important cause of chorioamnionitis. Arch Pathol Lab Med. 1985;109:739-743.
- Altshuler G, Hyde S. Clinicopathologic considerations of fusobacteria chorioamnionitis. Acta Obstet Gynecol Scand. 1988;67:513–517.
- Bohrer JC, Kamemoto LE, Almeida PG, Ogasawara KK. Acute chorioamnionitis at term caused by the oral pathogen Fusobacterium nucleatum. Hawaii J Med Public Health. 2012;71(10):280-281.
- Cartwright EJ, Jackson KA, Johnson SD, Graves LM, Silk BJ, Mahon BE. Listeriosis outbreaks and associated food vehicles, United States, 1998-2008. Emerg Infect Dis. 2013;19(1):1-9.
- Castellarin M, Warren RL, Freeman JD, et al. Fusobacterium nucleatum infection is prevalent in human colorectal carcinoma. Genome Res. 2012;22(2):299-306.
- Han YW, Redline RW, Li M, et al. Fusobacterium nucleatum induces premature and term stillbirths in pregnant mice: implication of oral bacteria in preterm birth. Infect Immun. 2004;72(4):2272-2279.
- Kraus FT, Redline RW, Gersell DJ, Nelson DM, Dicke JM. Inflammation and infection. In: Atlas of NonTumor Pathology - Placental Pathology,1st series, fascicle 3. Washington, DC: ARP Press; 2004:75-115.
- Stein A, Boubli L, Blanc B, Raoult D. Genital mycoplasmas in placental infections. Infect Dis Obstet Gynecol. 1994;1(6):275-281.
- Swidsinski A, Dörffel Y, Loening-Baucke V, et al. Acute appendicitis is characterised by local invasion with Fusobacterium nucleatum/necrophorum. Gut. 2011;60(1):34-40.
Author
2014
Megan K. Dishop MD
Surgical Pathology Committee
Department of Pathology, Children's Hospital Colorado
University of Colorado School of Medicine
Answer Key
- Candida albicans (a).
- Listeria monocytogenes (d).
- Fusobacterium nucleatum (b).