- Home
- Member Resources
- Pathology Case Challenge
- Pancreas copy
Clinical Summary
A 26-year-old woman sees her physician because of abdominal discomfort. She undergoes an extensive workup in which an 8.0 cm mass is identified in the uncinate process of the pancreas by computed tomography scan. She undergoes a resection.
Master List of Diagnoses
- Acinar cell carcinoma
- Mucinous cystic neoplasm
- Pancreatic adenocarcinoma
- Pancreatic neuroendocrine tumor
- Solid-pseudopapillary neoplasm
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2016, case 36, and is a solid-pseudopapillary neoplasm.
Criteria for Diagnosis and Comments
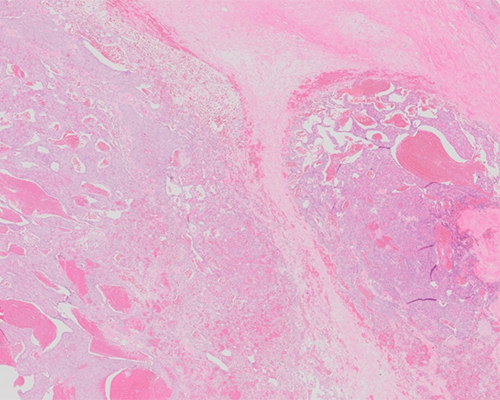
Sections demonstrate a histologically varied neoplasm with some sections showing adjacent pancreas. The tumor cells are small and monotonous with clear to eosinophilic cytoplasm. In some areas these cells are cohesive while in other areas they are dishesive. In some dishesive areas these cells form pseudopapillae by surrounding vessels that have adjacent hyalinized stroma making a rosette-like pattern. There are scattered areas of hemorrhage, cystic change, and aggregates of foamy macrophages. The nuclei are uniform with indistinct nucleoli. Some cells contain longitudinal grooves and only rare mitoses are present. Some sections contain aggregates of eosinophilic globules of varying size that are periodic acid Schiff (PAS) positive. These features are classic for solid-pseudopapillary neoplasm (SPN).
SPN is an uncommon tumor that accounts for 1% - 2% of all pancreatic neoplasms. SPN most commonly occur in females in their 20s (approximately 90%), and account for 30% of all pancreatic neoplasms in those under the age of 40. There has been a 7-fold increase in the number of cases detected since 2000, felt to be due to the increased use of abdominal imaging. There are no established clinical or genetic syndromes associated with SPN.
SPN can be found in any part of the pancreas and do not have a propensity for any certain region. It has rarely been reported outside the pancreas in peripancreatic tissue and in the mesocolon. SPN are usually grossly well-circumscribed and sometimes can have a fibrous capsule. Microscopically, however, they can infiltrate into the adjacent pancreatic tissue and on rare occasions infiltrate into adjacent organs. SPN can have a varied appearance as its name suggests. The more diminutive tumors tend to be more solid in nature. Larger tumors commonly have hemorrhage, necrosis, and cystic degeneration, which is the state at which most of these tumors are identified (average size, 8.0 – 10.0 cm). On cut surface these tumors tend to be soft with the solid areas being brown and yellow.
Microscopically these tumors tend to be varied containing solid, cystic and pseudopapillary areas. Hemorrhagic-necrotic areas are commonly present. The solid areas, present at the periphery of larger tumors, are composed of a monomorphic population of cells separated by small vessels. These vessels tend to have perivascular collagen deposition. The cells are small with uniform nuclei and indiscriminate nucleoli. Nuclear longitudinal grooves are a classic finding along with PAS-positive globules. These cells can either be cohesive or poorly cohesive. When these cells do disassociate, they can result in pseudopapillae. Microcalcifications and ossification can also be present. There are some rare histologic variants that include: clear cell, oncocytic, and pleomorphic (where more than 20% of the tumor has significant nuclear pleomorphism).
The immunohistochemical profile of SPN is unique for pancreatic neoplasms. There is strong nuclear expression of beta-catenin along with loss or abnormal cytoplasmic expression of E-cadherin. Keratin reactivity is usually absent or focal depending on the method of retrieval. These tumors show diffuse staining with vimentin and are also positive for CD10. The tumor can be focally positive for synaptophysin, but routinely negative for chromogranin. Trypsin and chymotrypsin are negative as well.
SPN are considered tumors of low malignant potential. Surgical resection is usually curative with only 10% - 15% recurring after complete surgical resection. Local dissemination has been reported after rupture and abdominal trauma. Of note, there are no proven morphologic predictors of outcome.
The main molecular pathway involved in SPN involves Wnt/beta-catenin. Most commonly it is due to point mutations within exon 3 of the CTNNB1 gene, which codes for beta-catenin. This results in a gain of function mutation that prevents beta-catenin degradation. This abnormal accumulation of beta-catenin binds to T-cell transcription factor/lymphoid enhancer-binding factor (LEF1) which then is abnormally translocated to the nucleus. This in turn induces numerous oncogenic genes and activation of the Wnt/beta-catenin pathway. LEF1 can be detected by immunohistochemistry in SPN with diffuse nuclear labeling which is a unique finding for pancreatic tumors. The only other pancreatic neoplasm that LEF1 nuclear labeling has been described in is pancreatoblastoma, where it is present in the squamous corpuscles. Mutations commonly found in ductal adenocarcinoma (KRAS, TP53, SMAD4/DPC4, and CDKN2A/p16) have not been reported in SPN. In fact, whole genome sequencing has demonstrated an average of only three nonsynonymous mutations per SPN. This mutation rate is the lowest among pancreatic neoplasms sequenced to date.
Clinically these tumors are most commonly found incidentally, but if symptoms are present, they usually are abdominal discomfort, early satiety, nausea, vomiting, and pain. These tumors are not associated with increased chromogranin or CA19-9 serum levels. Although there are hypotheses and theories, the cell origin for SPN remains elusive. There is varying evidence for acinar, ductal, and neuroendocrine derivation as well as pluripotent stem cells from the genital ridges.
The usual cast of pancreatic characters is present in the differential diagnosis for a SPN. A low-grade neuroendocrine tumor (NET) can histologically be quite similar to a SPN because of its monotonous cell populations. However, NET usually do not contain vascular cores, foamy macrophages, longitudinal nuclear grooves, and eosinophilic globules. The focal synaptophysin positivity may also lead to confusion but NET do not show nuclear beta-catenin positivity. Acinar cell carcinoma can have a varied appearance like SPN. However, acinar cells contain a prominent nucleolus and have finely granular cytoplasm due to zymogen granules. Acinar cell carcinomas are positive for trypsin and chymotrypsin, which are negative in SPN. Pancreatic adenocarcinoma does also come up in the differential because it creates a pancreatic mass. However, these two tumors involve primarily two different age groups and are histologically and immunohistochemically distinct. Mucinous cystic neoplasms are also histologically distinctive from SPN.
Supplementary Questions
- What is the typical immunoprofile of solid-pseudopapillary neoplasms?
- Vimentin-, chromogranin-, nuclear beta-catenin-
- Vimentin-, synaptophysin+, nuclear beta-catenin-
- Vimentin+, chromogranin+, nuclear beta-catenin+
- Vimentin+, synaptophysin-, nuclear beta-catenin+
- Mutations in what gene lead to abnormal accumulation of beta-catenin?
- CTNNB1
- KRAS
- LEF1
- MLH1
- TP53
- Solid-pseudopapillary neoplasms preferentially involve what part of the pancreas?
- Body
- Head
- No site predilection
- Tail
- Uncinate process
References
- Bosman, F, Carneiro F, Hruban R, Theise N. World Health Organization Classification of Tumours of Digestive System. Lyon, FR: IARC; 2010.
- Mas-Moya J, Singhi A. Immunohistochemistry as a surrogate to molecular diagnosis in pancreatic tumors. Diagn Histopathol. 2015;21(3):116–121.
- Park M, Lim JS, Lee HJ, Na K, et al. Distinct Protein Expression Profiles of Solid-Pseudopapillary Neoplasms of the Pancreas. J Proteome Res. 2015 7;14(8):3007-3014.
- Terris B, Cavard C. Diagnosis and molecular aspects of solid-pseudopapillary neoplasms of the pancreas. Semin Diagn Pathol. 2014;31(6):484-490.
Authors
2016
William V. Chopp, MD, FCAP
Surgical Pathology Committee
Michigan Pathology Specialists
Grand Rapids, MI
Aaron Auerbach, MD, MPH
Surgical Pathology Committee
The Joint Pathology Center
Silver Spring, MD
Answer Key
- Vimentin+, synaptophysin-, nuclear beta-catenin+ (d)
- CTNNB1 (a)
- No site predilection (c)