Clinical Summary
A 46-year-old woman presents with progressive hirsutism. Laboratory studies show an elevated serum testosterone level. Pelvic ultrasound demonstrates a slightly enlarged left ovary. Total hysterectomy, bilateral salpingo-oophorectomy, and omental and peritoneal biopsies are performed. Gross examination of the left ovary reveals a 3.8 x 3.5 x 3.4 cm well circumscribed tan-yellow nodule within the ovarian parenchyma. The external surface of the ovary is smooth and tan without disruption.
Master List
- Adult granulosa cell tumor
- Endometrioid adenocarcinoma, sertoliform variant
- Krukenberg tumor (metastatic adenocarcinoma)
- Sertoli cell tumor
- Sertoli-Leydig cell tumor
- Trabecular carcinoid tumor
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2013, case 39, and is a Sertoli-Leydig cell tumor.
Criteria for Diagnosis and Comments
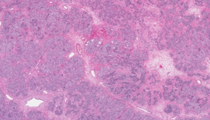
The histologic sections show fragments of ovarian tissue largely replaced by solid, cellular nodules with interspersed hyalinized or edematous stroma. These nodules consist primarily of dark, cuboidal to columnar Sertoli cells with somewhat vacuolated cytoplasm present in small nests, cords, and closed tubules. Occasional open or hollow tubules are present. These cells have relatively uniform nuclei with even, finely granular chromatin and small nucleoli. Few clusters show more spindled cell morphology. Scattered within the stroma are larger, polygonal Leydig cells with characteristic uniform, round nuclei with prominent nucleoli and abundant eosinophilic to clear cytoplasm. Within this cytoplasm, occasional yellow-brown lipochrome pigment is seen and rare slender, red-pink rods (Reinke crystalloids) may be identified. Mitotic activity is minimal. The findings are characteristic of a Sertoli-Leydig cell tumor.
Sertoli-Leydig cell tumors (SLCTs) are uncommon ovarian tumors with a peak incidence in the third decade of life. As in this case, up to 50% of patients present with androgenic manifestations such as virilism, amenorrhea, deepened voice, or clitoromegaly. Patients may also experience mass-related symptoms or abnormal uterine bleeding. The vast majority of SLCTs are unilateral with a mean size of 12.0-14.0 cm (ranging up to 35.0 cm). The cut surface is solid, yellow, and lobulated, with less differentiated tumors showing more areas of cysts, hemorrhage, and necrosis. Histologically the degree of differentiation is determined by the proportions of Leydig and spindle cells present as well as by the degree of tubular differentiation. Well differentiated tumors have well formed, open tubules and abundant Leydig cells; there is little nuclear atypia or mitotic activity. More commonly, accounting for two-thirds of SLCTs, the tumors are of intermediate or poor differentiation. Poorly differentiated SLCTs display a dominant spindle cell pattern (resembling primitive gonadal stroma), high nuclear grade, and sparse Leydig cells. The lobulated architecture may be lost in these tumors, and a diffuse pattern may be prominent. The presented slide shows a tumor of intermediate differentiation with only mild nuclear atypia and areas with readily identifiable Leydig cells; the Sertoli cells are arranged in clusters with minimal tubule development and a minor spindle cell component.
Although little is known about the pathogenesis of ovarian sex cord-stromal tumors, mutations in the DICER1 gene have recently been reported in ovarian SLCTs. This mutation is associated with the pleuropulmonary blastoma family tumor and dysplasia syndrome, which includes ovarian SLCT, nodular thyroid hyperplasia (multinodular goiter), cystic nephroma, nasal chondromesenchymal hamartoma, and ocular medulloepithelioma, among others.
The mortality rate associated with most SLCTs is low, partly due to the fact that most tumors present at early stage IA, with a lesion confined to the ovary. However certain histologic features, such as poor differentiation and tumor rupture, are associated with a more aggressive course. Additionally, intermediate and poorly differentiated SLCTs may contain heterologous elements which, when of mesenchymal origin, are also associated with the development of metastases. Complete surgical staging with total hysterectomy and bilateral salpingo-oophorectomy is recommended, although lymphadenectomy may be omitted. A woman with a desire to preserve fertility and a tumor confined to the ovary may be managed with unilateral salpingo-oophorectomy and observation; however completion surgery should be considered upon finishing childbearing. In cases where metastasis is present, adjuvant chemotherapy is generally recommended; however, clinical data demonstrating the benefits of such management is lacking.
SLCT may resemble other ovarian neoplasms in Leydig cell-poor areas. Although identification of Leydig cells is a helpful indicator of a SLCT, it is important to remember that primary or metastatic carcinomas of the ovary may undergo stromal luteinization resembling Leydig cells. Even pure Sertoli cell tumors may undergo rare stromal luteinization causing difficulty distinguishing from SLCT; however the presence of androgenic rather than estrogenic clinical manifestations, heterologous components, and more than rare cells consistent with Leydig cells supports the diagnosis of SLCT.
Adult granulosa cell tumors display trabeculae, cords, or a diffuse pattern which may mimic Leydig cell-poor regions of an intermediate or poorly differentiated SLCT. They may be distinguished from SLCTs by their longitudinal nuclear grooves and rosette arrangement of nuclei into Call-Exner bodies. In addition, keratin stain may aid in distinguishing these two lesions. When adult granulosa cell tumors express keratin, a paranuclear punctate pattern is seen. SLCTs are variably positive for keratins, however when present show a diffuse cytoplasmic staining pattern.
Endometrioid adenocarcinomas of the ovary may display epithelial cells which form small glands, hollow tubules, or solid tubular structures in a fibromatous background. As the name suggests, this "sertoliform" variant mimics well differentiated SLCT. These tumors are particularly prone to stromal luteinization, furthering the potential diagnostic dilemma. Thorough sampling should reveal glands with more classic-appearing well differentiated endometrioid morphology and perhaps squamous differentiation. Endometrioid adenocarcinoma is frequently associated with endometriosis and is bilateral in approximately 28% of cases. Additionally, endometrioid adenocarcinoma is immunoreactive with epithelial membrane antigen (EMA) and negative for inhibin, while the reverse is characteristic of SLCT.
A Krukenberg tumor's nodular architecture, stromal edema, and occasional lack of overt signet ring cell morphology may show a similar low-power pattern to SLCTs. However, closer examination should reveal cytoplasmic mucin in Krukenberg tumors, and Leydig cells in SLCTs. Krukenberg tumors are generally bilateral (greater than 70% of cases) and will be positive for mucicarmine stain, highlighting signet ring cells, while negative for inhibin. The overwhelming majority of SLCTs are unilateral and these tumors are inhibin-positive while negative for mucin stains.
Carcinoid tumors with a trabecular arrangement may mimic the open Sertoli cell tubules seen in well-to-intermediately differentiated SLCTs. Stromal luteinization is also commonly seen in trabecular carcinoids. These tumors may be distinguished from SLCTs by their diffuse positivity for at least one neuroendocrine marker, lack of inhibin staining, and associated mature cystic teratoma (present in approximately 60% of cases).
Supplementary Questions
- Which of the following ovarian tumors is most likely to be bilateral?
- Adult granulosa cell tumor
- Endometrioid adenocarcinoma
- Krukenberg tumor
- Sertoli-Leydig cell tumor
- Trabecular carcinoid
- Which of the following histologic features are typically displayed in well-differentiated Sertoli-Leydig cell tumors?
- Abundant spindled cells
- Developed tubules
- Heterologous elements
- Rare Leydig cells
- Significant nuclear atypia
- An immunoprofile of chromogranin-negative, EMA-positive, inhibin-negative, keratin-positive is most likely seen in which of the following ovarian tumors?
- Adult granulosa cell tumor
- Endometrioid adenocarcinoma
- Krukenberg tumor
- Sertoli-Leydig cell tumor
- Trabecular carcinoid
References
- Frio TR, Bahubeshi A, Kanellopoulou C, et al. JAMA. 2011;305:68-77.
- Hervai-Moussavi A, Anglesio MS, Cheng SWG, et al. NEJM. 2012;366:234-242.
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Ovarian Cancer including fallopian tube cancer and primary peritoneal cancer, version 1.2013. http://www.nccn.org. Accessed January 30, 2013.
- Oliva E, Alvarez T, Young RH. Sertoli cell tumor of the ovary. A clinicopathologic and immunohistochemical study of 54 cases. Am J Surg Pathol. 2005;29:143-156.
- Robboy SJ, Mutter GL, Prat J, Bentley RC, Russell P, Anderson MC, eds. Ovarian sex cord-stromal and steroid cell tumors. In: Robboy's Pathology of the Female Reproductive Tract. 2nd ed. Churchill Livingstone, Elsevier Ltd; 2009.
- Tavassoli FA, Mooney E, Gersell DJ, et al. Sex cord-stromal tumours. In: Tavassoli FA, Devilee P, eds. World Health Organization Classification of Tumours. Pathology and Genetics. Tumours of the Breast and Female Genital Organs. IARC Press; 2003:146-161.
- Thrall MM, Paley P, Pizer E, Garcia R, Goff BA. Patterns of spread and recurrence of sex cord-stromal tumors of the ovary. Gynecol Oncol. 2011;122:242-245.
- Young RH. Sex cord-stromal tumors of the ovary and testis: their similarities and differences with consideration of selected problems. Mod Pathol. 2005;18:S81-S98.
- Zaloudek C, Norris HJ. Sertoli-Leydig tumors of the ovary. A clinicopathologic study of 64 intermediate and poorly differentiated neoplasms. Am J Surg Pathol.1984;8:405-417.
Author
2013
Rochelle A. Simon, MD FCAP
Surgical Pathology Committee
Women & Infants Hospital of Rhode Island,
Alpert Medical School of Brown University
Providence, RI
Answer Key
- Krukenberg tumor (c).
- Developed tubules (b).
- Endometrioid adenocarcinoma (b).