- Home
- Member Resources
- Pathology Case Challenge
- Mesenteric Lymph Node
Clinical Summary
A 52-year-old woman was diagnosed with invasive rectal adenocarcinoma on a recent colonoscopy. At laporatomy, an incidental firm 8.0 x 6.0 x 4.0 cm rounded mass is identified in the mesentery. Sections of the mass are submitted for flow cytometric, microscopic, and immunohistochemical analysis. Immunohistochemical studies reveal scattered larger cells are positive for CD45, CD20, CD79a, bcl-6, and EMA (weak). They are negative for CD30, CD15, and EBV-associated latent membrane protein (LMP). CD21 reveals scattered follicular dendritic meshworks. Other immunohistochemical and flow cytometric studies reveal a T-cell dominant profile, a small subset of which are positive for CD57.
Master List
- Follicular lymphoma
- Nodular lymphocyte-predominant Hodgkin lymphoma
- Nodular sclerosis classical Hodgkin lymphoma
- Reactive follicular hyperplasia
- T-cell/histiocyte rich large B-cell lymphoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2013, case 32, and is nodular lymphocyte-predominant Hodgkin lymphoma.
Criteria for Diagnosis and Comments
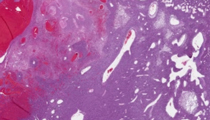
Histologic sections show an effaced lymph node with a predominantly small lymphoid infiltrate. Scattered histiocytes and larger atypical cells are present. These larger cells show irregular nuclear contours and prominent nucleoli, and rare cells resemble Reed-Sternberg (RS) cells. A vague nodular architecture is present, though depending on the section received it may not be readily apparent. The combined morphologic and immuhistochemical findings (as detailed above) are diagnostic of nodular lymphocyte-predominant Hodgkin lymphoma.
Nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL) is a distinct clonal B-cell neoplasm. It shares some characteristics with classical Hodgkin lymphoma. Its distinct classification is relatively recent, as it has been confused in the past with lymphocyte-rich classical Hodgkin lymphoma (CHL) and T-cell/histiocyte rich large B-cell lymphoma (THRLBCL).
NLPHL comprises approximately 5% of all Hodgkin lymphoma cases. Like its classical (CHL) counterpart, it is primarily a nodal-based disease and commonly involves the cervical chain, though mediastinal, splenic, and bone marrow involvement are rare. NLPHL also can involve axillary, inguinal, and abdominal lymph nodes. The lymphoma is most common in the 30-50 year old range, and there is a male predominance.
NLPHL usually develops slowly, and despite fairly common recurrences, has a good prognosis. In lower stage disease, the prognosis is excellent. In some cases, resection can be curative. Progression to diffuse large B-cell lymphoma is rare but does occur (~3-5% of cases, but has been reported as high as 10%).
The typical morphologic picture of NLPHL consists of a lymph node effaced by a nodular proliferation of small lymphocytes, histiocytes, and large lymphoid cells. These larger cells are clonal and always in the minority, and they show a relatively broad morphologic spectrum. They typically have one large nucleus that is extremely folded or even multilobated; this is termed a lymphocyte-predominant ('LP', formerly known as 'L&H') or 'popcorn' cell. The cells can have prominent and multiple nucleoli, though they are usually not as prominent as a typical RS cell. However, they can rarely be indistinguishable from an RS cell. Although the predominant morphologic pattern is nodular, more diffuse areas can be found, which are comprised of lymphocytes and histiocytes. Uncommonly, diffuse areas predominate. In these cases, the typical morphologic findings of NLPHL can be difficult to identify. Other morphologic patterns of NLPHL have been described. Some cases show adjacent reactive follicular hyperplasia which can be involved by what has been termed 'progressive transformation of germinal centers' (PTGC). These are enlarged nodules comprised predominantly of small lymphocytes with scattered larger centroblast-like cells. PTGC may precede a diagnosis of NLPHL, though it is uncertain if this is a pre-neoplastic phenomenon.
Immunophenotypic studies confirm a germinal center B-cell derivation for LP cells. However, the typical immunophenotypic pattern is distinct from classical Hodgkin lymphoma. The cells are usually positive for CD45, CD20, CD79a, and bcl-6. EMA is occasionally positive. Only rare cases are positive for CD30 and CD15; latent EBV infection is consistently absent. The opposite immunoprofile is usually seen in classical Hodgkin lymphoma, though there is some overlap. LP cells are usually ringed by CD57+ T-cells, and these rosettes can be well-visualized by immunohistochemical studies. The recognition of the nodular architecture is essential for the diagnosis, and can be aided by CD21 staining of follicular dendritic meshworks. Currently, the recognition of only one nodule with the typical features of NLPHL, even in a diffuse background, is sufficient to rule out a primary THRLBCL. If a nodular architecture is not identified, then diffuse large B-cell lymphoma (typically THRLBCL) enters the differential. Even in a nodular background, increased numbers of LP cells in extrafollicular areas has been associated with an increased risk of transformation to diffuse large B-cell lymphoma.
The prominent nodular architecture of NLPHL raises the differential diagnostic consideration of another B-cell lymphoma, follicular lymphoma. Follicular lymphoma can rarely have larger cells with multilobated nuclei within the follicles, which can resemble LP cells. Given that LP cells are usually positive for bcl-6, this may cause some confusion. However, an extended immunohistochemical panel will reveal a B-cell dominant population within the follicles that co-expresses CD10 and BCL2, which is not seen in NLPHL.
NLPHL can rarely present with sclerosis, which can become more common with recurrences. This may cause confusion with nodular sclerosis classical Hodgkin lymphoma. The lack of a pleomorphic infiltrate, typical lacunar cell population, and different immunohistochemical profile will be helpful in differentiating between the two.
Reactive follicular hyperplasia can involve an entire node and simulate a neoplastic process. Scattered germinal centers can be seen in NLPHL, though these are typically in the minority. Reactive follicular hyperplasia shows numerous reactive germinal centers, allowing it to be distinguished from NLPHL in most instances.
Perhaps one of the most important differential diagnoses of NLPHL (and potentially the most difficult to separate) is THRLBCL. Given that the neoplastic B-cells in both NLPHL and THRLBCL comprise a minority of the cellularity (in a background of numerous T-cells), they can be confused with each other. The neoplastic B-cells in THRLBCL can mimic LP cells, and can show a similar immunoprofile. Further complicating this differential is that when NLPHL recurs, it can resemble THRLBCL. As discussed above, recognition of a nodular architecture is essential in differentiating between the two. Recognition of this can be aided by CD21 immunohistochemical staining.
Supplementary Questions
- Mediastinal involvement is relatively common in nodular lymphocyte-predominant Hodgkin lymphoma.
- True
- False
- What is the typical immunoprofile of the lymphocyte predominant (LP)/'popcorn cell'?
- CD45-, CD20-, CD30+, CD15+
- CD45+, CD20+, CD30-, CD15-
- CD45+, CD20+, CD30+, CD15-
- CD45+, CD20-, CD30+, CD15-
- CD45-, CD20-, CD30+, CD15-
- Which of the following is correct about nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL)?
- It has a good prognosis, especially in lower stage disease burden
- It is associated with EBV infection
- It is more common than classical Hodgkin lymphoma
- It never transforms into diffuse large B-cell lymphoma
- Reed-Sternberg cells are commonly seen
References
- Biasoli I, Stamatoullas A, Meignin V, et al. Nodular, lymphocyte-predominant Hodgkin lymphoma: A long-term study and analysis of transformation to diffuse large B-cell lymphoma in a cohort of 164 patients from the Adult Lymphoma Study Group. Cancer. 2010;116:631-639.
- Fan Z, Natkunam Y, Bair E, et al. Characterization of variant patterns of nodular lymphocyte predominant Hodgkin lymphoma with immunohistologic and clinical correlation. Am J Surg Pathol. 2003;27:1346-1356.
- Swerdlow S, Campo E., Harris N, et al (eds). WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (4th ed.). Lyon, France: IARC Press;2008.
- Uherova P, Valdez R, Ross C, et al. Nodular lymphocyte predominant Hodgkin lymphoma: an immunophenotypic reappraisal based on a single-institution experience. Am J Clin Pathol. 2003;119(2):192-198.
Author
2013
Brad Bryan, MD, FCAP
Surgical Pathology Committee
Central Oregon Pathology Consultants
Bend, OR
Answer Key
- False (b).
- CD45+, CD20+, CD30-, CD15- (b).
- It has a good prognosis, especially in lower stage disease burden (a).