Clinical Summary
A 41-year-old woman presents with a one-month history of vague abdominal pain. Physical examination reveals mild right-upper quadrant tenderness. Computerized tomography (CT) imaging shows a solitary 12 cm cyst in the left lobe of the liver. No other imaging abnormalities are present in the chest, abdomen, or pelvis. Her serum alpha-fetoprotein, CEA, and CA19-9 are within normal limits.
Master List
- Ciliated hepatic foregut cyst
- Cystic cholangiocarcinoma
- Hepatic endometriosis
- Hepatobiliary cystadenoma
- Intraductal papillary neoplasm of the bile duct
- Simple biliary cyst
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2015, case 19 and is a hepatobiliary cystadenoma.
Criteria for Diagnosis and Comments
Hepatobiliary cystadenomas (HBCs) are rare indolent cystic neoplasms principally of the liver, but can occasionally arise in the gallbladder and extrahepatic biliary tree. They typically present as large central or left-sided solitary cysts in young and middle-aged women (range 2 to 87 years, median of 45 years, female: male 20:1). They may be clinically silent but when symptomatic abdominal pain is the most common symptom, with only a minority (roughly 5%) being associated with more serious complications including bleeding, infection, rupture and exceptionally malignant degeneration. The pathologic features, clinical behavior and demographics of HBCs are very similar to mucinous cystic neoplasms of the pancreas and because of this, HBCs are often referred to as mucinous cystic neoplasms of the liver. There is no association with primary liver or biliary disease (e.g. viral hepatitis, intrahepatic stones, cirrhosis, etc.).
HBC is typically large but can range from just a few centimeters to over 20 cm in size. Ultrasound and CT imaging demonstrates a cyst with a thick external wall, multiloculation with internal septation of variable degree, and less frequently calcification, mural nodularity, and papillary projections; the latter two may herald the rare malignant degeneration of these lesions. Cyst fluid is typically clear and watery but can be mucinous, and rarely purulent or hemorrhagic.
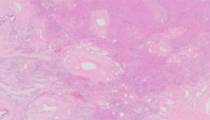
To reliably find the characteristic histopathologic features generous sampling is generally recommended. The inner lining of the cysts is typically flat, although papillary structures may be occasionally seen, and is predominantly composed of columnar and cuboidal mucus secreting epithelial cells that may be attenuated in areas (particularly if previously biopsied or aspirated). Gastric, intestinal and squamous metaplasia as well as dysplasia may be seen. Underlying this epithelium is an ovarian-type stroma, which appears as a band of closely pack spindle cells of variable abundance that may be luteinized or associated with a xanthogranulomatous reaction. Immunohistochemistry, which is generally not required to make the diagnosis, shows the epithelial component to have an immunohistochemical profile like that of the biliary tree (positive for cytokeratins 7 and 19) and the ovarian stromal component to label for estrogen, progesterone and inhibin. Features of malignant degeneration include severe cytologic atypia, mitotic activity and stromal invasion.
Due to the potential of serious complications associated with HBC complete surgical resection is the generally recommended management. Unroofing and other modalities that provide only partial resection are associated with a 50% local recurrence rate and are thus felt to be inadequate treatment for HBC.
Since diagnosing HBC via needle biopsy or aspirate is difficult due to the low probability of obtaining ovarian-type stroma and, cyst fluid analysis for CA 19-9 and carcinoembryonic antigen has only mixed results at differentiating HBC from its mimics, a presumptive preoperative diagnosis of HBC often relies largely on imaging. A definitive diagnosis however often requires histologic evaluation of resected material at frozen section ideally (to help guide surgical management) or on permanent sections.
When considering the differential diagnosis it is important to note that while HBC has several distinguishing features, the most helpful is the presence of ovarian-type stroma, which is not seen in other cystic liver lesions.
The first differential diagnostic consideration to keep in mind is a simple biliary cyst which is by far the most common cystic lesion of the liver (may be present in 20% of the adult population). Like HBC, simple biliary cysts are often incidental, but unlike HBC, simple biliary cysts are often small, multifocal, unilocular and have no malignant potential. Simple biliary cysts are lined by cuboidal or flattened epithelium and lack subjacent ovarian-type stroma. When complications necessitate treatment simple biliary cysts require only simple unroofing, not complete resection.
Ciliated foregut cysts are common in the tracheal-bronchial tree and esophagus but are only rarely seen in the liver. As their name implies ciliated hepatic foregut cysts are lined by ciliated pseudostratified columnar epithelium with no associated ovarian-type stroma.
Intraductal papillary neoplasm of the bile duct (IPNB) may be cystic but unlike HBC, IPNB are intraductal lesions that communicate with the biliary tree, show a predominantly papillary architecture, lack the ovarian-type stroma and are frequently associated with an invasive adenocarcinoma (malignant degeneration is seen in nearly half of cases of IPNB). Cystic cholangiocarcinoma can be distinguished from HBC as it typically shows cytologically malignant epithelium and stromal invasion.
Hepatic intraparenchymal endometriosis is very rare, it may mimic HBC macroscopically as it can manifest as a cystic tumor with a thick wall and complex multiloculation. It may be seen with or without a history of pelvic endometriosis. The familiar histologic features of endometriosis make for a clear distinction from HBC; hepatic endometriosis demonstrates typical endometrial glands admixed with endometrial stroma and hemorrhage.
Supplementary Questions:
- Which of the following is true regarding the imaging characteristics of hepatobiliary cystadenomas?
- Multifocal, multilocular with direct communication to the biliary tree
- Multifocal, unilocular, and may contain calcifications
- Solitary, multilocular, and may contain mural nodules
- Solitary, solid, and cystic
- Solitary, unilocular, and may contain papillary structures
- What is the single most useful histologic feature to separate hepatobiliary cystadenoma from its differential diagnostic considerations?
- Cellular atypia
- Columnar epithelial lining
- Cytokeratin 7 immunohistochemical labeling
- Ovarian-type stroma
- Stromal invasion
- Which of the following is true regarding the management of hepatobiliary cystadenomas?
- Complete resection provides adequate therapy.
- Liver transplant provides the only definitive treatment due to high rate of recurrence.
- Neoadjuvant chemotherapy followed by complete resection is the generally recommended treatment.
- Partial resection via unroofing provides adequate therapy.
- Percutaneous drainage provides adequate therapy.
References
- Abdul-Al HM, Makhlouf HR, Goodman ZD. Expression of estrogen and progesterone receptors and inhibin-alpha in hepatobiliary cystadenoma: An immunohistochemical study. Virchows Archiv: An International Journal of Pathology. 2007;450(6):691-697.
- Devaney K, Goodman ZD, Ishak KG, Kamal G. Hepatobiliary cystadenoma and cystadenocarcinoma. A light microscopic and immunohistochemical study of 70 patients. Am J Surg Pathol. 1994;18(11):1078-1091.
- Fuks D, Voitot, H, Paradis V, Belghiti J, Vilgrain V, Farges O. Intracystic concentrations of tumour markers for the diagnosis of cystic liver lesions. Brit J Surg. 2014;101(4):408-416.
- Goldsmith PJ, Ahmad N, Dasgupta D, Campbell J, Guthrie JA, Lodge JP. Case of hepatic endometriosis: A continuing diagnostic dilemma. HPB Surgery. 2009:407206.
- Martel G, Alsharif J, Aubin JM, et al. (2013). The management of hepatobiliary cystadenomas: lessons learned. HPB. 2013;15(8):617-622.
- Tsui WMS, Adsay NV, Crawford JM, Hruban RH, Kloppel G, Wee A. Mucinous cystic neopolasms of the liver. In Bosman FT, Carneiro F, Hruban RH, Theise ND, eds. WHO Classification of Tumours of the Digestive System, 4th ed. Lyon, FR: International Agency for Research on Cancer;2010:236.
- Vick DJ, Goodman ZD, Deavers MT, Cain J, Ishak KG. Ciliated hepatic foregut cyst: A study of six cases and review of the literature. Am J Surg Pathol. 1999;23(6):671-677.
- Yeh MK. Benign and malignant tumors of bile ducts. In Saxena R, ed. Practical Hepatic Pathology Philadelphia, PA: Elsevier; 2011:506-508.
- Zen Y, Jang KT, Ahn S, et al.. Intraductal papillary neoplasms and mucinous cystic neoplasms of the hepatobiliary system: Demographic differences between Asian and western populations, and comparison with pancreatic counterparts. Histopathology. 2014;65(2):164-173.
Author
H. Parry Dilworth, MD
Surgical Pathology Committee
Hospital Pathology Associates
Minneapolis, MN
Answer Key
- Solitary, multilocular, and may contain mural nodules (c)
- Ovarian-type stroma (d)
- Complete resection provides adequate therapy. (a)