Clinical Summary
A 42-year-old woman presents with right upper quadrant pain. Physical examination reveals no abnormalities. Her laboratory evaluation is remarkable for a 2-fold increase in alkaline phosphatase, but otherwise normal liver function tests and a normal complete blood count. Computed tomography (CT) scan shows multiple nodular lesions involving her entire liver. These lesions are hypoechoic on liver ultrasound. Given the imaging findings, serum tumor markers are evaluated including alpha-fetoprotein, carcinoembryonic antigen, CA19-9, CA125 and CA27-29, all of which are normal. She undergoes wedge biopsy of one of the liver nodules and subsequently undergoes orthotopic liver transplantation. The gross examination of the explanted liver shows the entire liver to be involved by multiple grey-white ill-defined nodules ranging from 0.5 cm – 10.0 cm and replacing about half of the liver parenchyma. The slide presented is comprised of a representative nodule from the explanted liver.
Master List
- Angiosarcoma
- Cholangiocarcinoma
- Cirrhosis
- Hepatic epithelioid hemangioendothelioma
- Metastatic signet ring cell carcinoma
- Sclerosed hemangioma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2014, case 11 and is a hepatic epithelioid hemangioendothelioma.
Criteria for Diagnosis and Comments
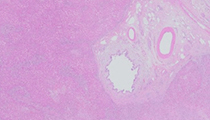
The liver nodule shows abundant myxohyaline and sclerotic stroma with prominent thin walled non-atypical vasculature. Populating this stroma is a cellular infiltrate of two types: spindled (dendritic) cells with long branching processes and rounded epithelioid cells that frequently have a central vacuole, some containing red blood cells. Cellular atypia is mild and mitotic figures are rare. The liver acinar parenchyma is entirely replaced by this lesion; however, close examination reveals infiltrative growth encompassing pre-existing portal triads within the mass lesion, including intravascular growth. These histologic features are characteristic of hepatic epithelioid hemangioendothelioma (HEH), a diagnosis that should be confirmed with immunohistochemical labeling for vascular markers (such as factor VIII-related antigen, CD31, CD34 and D2-40).
Epithelioid hemangioendothelioma is an uncommon vascular neoplasm that may develop in soft tissue, lung, bone, brain, liver and small intestine. It has malignant potential with a variable clinical course but almost always follows a less aggressive course than angiosarcoma. It was first described by Weiss and Enzinger in 1982 in a series of soft tissue tumors.
The hepatic form, HEH, is rare with an incidence of one per million population. It has a peak incidence in adults between 30 and 40 years of age and is slightly more common in women with a female to male ratio of 3:2. No clear risk factors have been identified. Presenting signs and symptoms are widely varied and 25% of patients are asymptomatic. Of symptomatic patients, the most common symptoms in order of frequency are abdominal pain, hepatomegaly, and weight loss. Uncommon presentations (less than 10% of patients) include anorexia, ascites, nausea/vomiting, and jaundice. This lesion is rarely associated with cirrhosis.
The prognosis, while generally intermediate, is widely variable ranging from long term survival to a small minority succumbing to disease within weeks of diagnosis. Metastatic disease is relatively common, occurring in one quarter of patients, but it is not necessarily correlated with a poor prognosis.
HEH shows a range of changes on CT scan but it is almost always seen as multiple lesions that tend to be peripheral with liver capsule retraction. The lesions typically begin as distinct nodules and, with more advanced disease, these nodules coalesce to form larger masses. CT scan with contrast shows peripheral enhancement with variable enhancement in the tumor centers. These lesions are predominantly hypoechoic on ultrasound examination with no blood flow on Doppler studies. The constellation of radiographic features of HEH is similar to those of peripheral cholangiocarcinoma, treated hepatocellular carcinoma, and large atypical cavernous hemangioma.
No standard treatment protocols exist, however, the most common and effective treatments are surgical, including orthotopic liver transplantation (LTx) and partial liver resection (LRx). LTx has been performed in 45% of published series of HEH patients with long term survival in 77% of patients; living liver donor transplants have been performed in a handful of patients with subsequent long term survival as well. LRx provides even better survival statistics with 95% long term survivors, however only 10% of HEH patients are eligible for LRx as the majority of HEH patients present with diffuse hepatic disease. A myriad of other therapies have been used in HEH including chemotherapy, radiotherapy and loco-regional treatments. Discussion of these modalities is beyond the scope of this format, but it can be summarized that these non-surgical treatments are of little value, especially as first-line therapies. While patients receiving no treatment have rarely experienced long term survival, including partial and even complete spontaneous regression of these lesions, an overall mortality of greater than 50% in this untreated patient group argues against observation only in most HEH patients.
An important differential diagnostic consideration with HEH is angiosarcoma (AS). This is a vital distinction as the prognosis of AS is almost invariably dismal with an average survival of 6 months, and patients with AS are not candidates for LTx. AS will label for the same vascular markers as HEH, but can be defined by its more severe cellular atypia, mitotic activity (including atypical mitoses), and necrosis. More poorly differentiated areas of AS closely resemble carcinomas with areas of papillary or solid growth of neoplastic cells.
Hemangiomas are the most common tumor of the liver and are composed of thin walled vascular channels, an appearance that generally would not enter into the histologic differential diagnosis of HEH. However, hemangiomas often undergo fibrosis and begin to resemble a scar (termed "sclerosed hemangioma"). Sclerosed hemangiomas may resemble HEH due to the similar appearing stromal component but can be distinguished from HEH by the absence of the dendritic and epithelioid components that characterize HEH.
Metastatic carcinomas (including signet ring cell carcinoma) and primary cholangiocarcinoma have destructive growth patterns that generally don't spare portal tracts (that is portal tracts don’t get incorporated into the tumor as they do in HEH). Additionally, these carcinomas do not have the characteristic intracellular lumina seen in the epithelioid cells of HEH; the mucin vacuoles of signet ring cells may mimic these lumina, however in signet cells, mucin vacuoles will be positive for mucin markers (like mucicarmine), and do not label with vascular markers. Cytokeratin immunohistochemistry will strongly label carcinomas but this is not particularly helpful in the differential of HEH as both the dendritic and epithelioid cells of HEH can be cytokeratin positive.
HEH is a tumefactive process replacing most or all of the liver acinar parenchyma, something that is not seen in cirrhosis, which retains much of the acinar parenchyma.
Supplementary Questions:
- Which of the following is a marker of hepatic epithelioid hemangioendothelioma?
- Cytokeratin AE1/AE3
- Factor VIII-related antigen
- HepPar1
- Kaposi sarcoma-associated herpes virus (HHV-8)
- Mucicarmine
- Hepatic epithelioid hemangioendothelioma is most common in older men.
- True
- False
- What constellation of features is most consistent with hepatic epithelioid hemangioendothelioma?
- Destructive growth, diffuse cytokeratin labeling, and low mitotic rate
- Epithelioid cells with intracellular lumina, hyalinized stroma, and marked atypia
- Factor VIII-related antigen labeling, minimal atypia, and brisk mitotic rate
- Hyalinized stroma, factor VIII-related antigen labeling, and low mitotic rate
- Sheets of atypical neoplastic cells, atypical mitoses, and necrosis
References
- Azzam RI, Alshak NS, Pham HP. AIRP best cases in radiologic-pathologic correlation: Hepatic epithelioid hemangioendothelioma. Radiographics. 2012;32(3):789-794.
- Ishak KG, Sesterhenn IA, Goodman ZD, Rabin L, Stromeyer FW. Epithelioid hemangioendothelioma of the liver: A clinicopathologic and follow-up study of 32 cases. Hum Pathol. 1984;15(9):839-852.
- Makhlouf HR, Ishak KG, Goodman ZD. Epithelioid hemangioendothelioma of the liver: A clinicopathologic study of 137 cases. Cancer. 1999;85(3):562-582.
- Mehrabi A, Kashfi A, Fonouni H, et al. Primary malignant hepatic epithelioid hemangioendothelioma: A comprehensive review of the literature with emphasis on the surgical therapy. Cancer. 2006;107(9):2108-2121.
Authors
2014
Joel Money, BA
Pathologist Aide
Hospital Pathology Associates
Minneapolis, MN
H. Parry Dilworth, MD, FCAP
Surgical Pathology Committee
Hospital Pathology Associates
Minneapolis, MN
Answer Key
- Factor VIII-related antigen (b).
- False (b).
- Hyalinized stroma, factor VIII-related antigen labeling, and low mitotic rate (d).