- Home
- Member Resources
- Pathology Case Challenge
- Left Internal Iliac Lymph Node
Clinical Summary
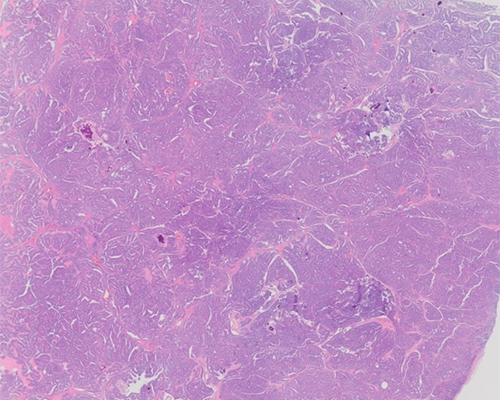
A 62-year-old man presents with an incidental finding of an enlarged lymph node along the left internal iliac chain. The patient has no prior history of malignancy. Laboratory findings include a normal complete blood count and serum levels in the normal reference range for PSA (2.8 ng/mL), carcinoembryonic antigen (2.5 mcg/L), and CA 19-9 (12 U/ml). Exploratory laparotomy with excision of the lymph node is performed. In addition to evaluation of H&E stained slides, a battery of immunohistochemical markers is applied, which shows the neoplastic cells to label for prostate-specific antigen (PSA) (focal cytoplasmic) and NKX3-1, with no labeling for cytokeratin 7 (CK7), cytokeratin 20 (CK20), CDX-2, chromogranin, synaptophysin, or thyroid transcription factor-1.
Master List of Diagnoses
- Metastatic bladder adenocarcinoma
- Metastatic colonic adenocarcinoma
- Metastatic pancreatic adenocarcinoma
- Metastatic prostatic adenocarcinoma
- Metastatic well-differentiated neuroendocrine tumor
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2016, case 38, and is a metastatic prostatic adenocarcinoma.
Criteria for Diagnosis and Comments
These findings are diagnostic of metastatic prostatic adenocarcinoma (PCa) based on the histomorphology in conjunction with the immunohistochemical labeling profile. The histomorphology alone is diagnostic of a carcinoma of unknown primary (CUP). The presence of CUP is a diagnostic challenge commonly encountered by pathologists. The practical importance of identifying a specific primary site is increasing with the development of targeted therapies. The labeling pattern of CK7(-)/CK20(-) narrows down the diagnosis as this pattern is the most commonly seen in prostatic, hepatocellular, renal cell, and adrenal cortical carcinomas. The definitive diagnosis of metastatic PCa is made based on the positive labeling for prostate specific immunohistochemical markers PSA and transcription factor NKX3-1.
PCa is typically gland-forming, like the example here, and shows regular glands with monotonous round nuclei containing prominent nucleoli with rare apoptotic bodies and rare mitotic figures. Typically, PCa has glands with straight luminal borders and lumina that contain crystalloids (dense eosinophilic crystal-like structures within lumina) and blue tinged mucin. PCa with loss of differentiation forms cribriform structures, fused glands, solid sheets/cords, and single cells. A minority (5% - 10%) of prostate adenocarcinomas are composed of distinct histologic variants including atrophic, pseudohyperplastic, microcystic, foamy gland, mucoid, and signet ring cell.
PSA like other cytoplasmic proteins associated with site-specific functions lose sensitivity with poor differentiation. The sensitivity of PSA is > 90% but the extent of labeling may only be focal in metastatic lesions as described in this case. Prostate specific acid phosphatase (PSAP) is another commonly used cytoplasmic protein target and has similar performance characteristics as PSA. NKX3-1 is a homeobox transcription factor whose expression is restricted to the prostate and has been shown to be a very sensitive and specific (> 90%) marker of PCa. While PSA and NKX3-1 are highly specific in identifying prostatic origin, exceptionally they can be positive in breast carcinoma and PSA may be positive in salivary gland neoplasms. Sensitivities for PSA and NKX3-1 are lower in some PCa variants, such as small cell carcinomas of the prostate.
Primary bladder adenocarcinoma is rare, with the majority associated with a history of congenital bladder exstrophy. Adenocarcinoma in the bladder is more typically due to secondary involvement from the colorectum or prostate. The majority of bladder adenocarcinomas are either mucinous, enteric (ie, look like colon adenocarcinoma), signet-ring cell or a mixture of these morphologies. While prostatic adenocarcinoma is often not a differential diagnostic problem, if there is histomorophologic overlap, the immunohistochemical profile can separate prostatic from bladder adenocarcinoma. The CK7/CK20 profile for bladder adenocarcinoma is not entirely consistent but most cases are CK20 positive with variable CK7 labeling. Most helpful in this differential diagnosis is the absence of both PSA and NKX3-1 in bladder adenocarcinoma.
Neither the histomorphology nor immunohistochemical pattern here is typical of colorectal adenocarcinoma. Colorectal adenocarcinoma is typically composed of irregular glands lined with columnar cells, abundant mitosis and apoptosis, and tumor necrosis. Colorectal adenocarcinoma in almost all cases shows strong diffuse CDX-2 and CK-20 labeling, with no labeling for PSA or NKX-3.
Pancreatic adenocarcinoma does not label with prostate markers PSA or NKX3-1, and in almost all cases shows strong diffuse CK7 labeling.
Midgut and hindgut well-differentiated neuroendocrine tumors (NETs) can present with nodal metastases in this region and do typically share some histomorphologic features with PCa including round regular nuclei and infrequent mitotic figures, only rare apoptotic bodies, and absent or minimal tumor necrosis. PCa however typically has prominent nucleoli not seen in well-differentiated NET. Immunohistochemistry is distinctive with NET being negative for prostate immunohistochemical markers PSA and NKX3-1, and positive for synaptophysin and, in most sites, chromogranin (hind gut carcinoids [rectum] are negative for chromogranin). A primary prostatic NET is extremely rare, but it too will share immunohistochemical markers with other NETs, including being negative for PSA.
PCa is the most commonly diagnosed life-threatening cancer in men with the lifetime risk of 1 in 6, and the risk of dying from prostate cancer is 1 in 35. As no PSA level cut-off level provides both high sensitivity and high specificity and specifically, there is no level that is low enough to entirely exclude the presence of prostate cancer (as illustrated in this patient). The utility of using serum PSA alone as a screening test has generally fallen out of favor. The role of PSA testing is in evolution, but currently it is (1) used with several other variables to assess the need for biopsy, (2) used with stage, histologic grade (Gleason score) for prognosis, and (3) as a tumor marker to monitor for recurrent disease, among other uses.
It is generally accepted that no imaging technique exists which is effective at evaluating the extent of prostatic involvement or the presence of extra-prostatic microscopic foci of PCa in men with low- and intermediate-risk disease. Metastatic prostate carcinoma most commonly involves regional lymph nodes (as present in this case) and bones of the axial skel¬eton where a characteristic osteoblastic response is often elicited. Despite the propensity to metastasize to bone, bone scans are not generally recommended in patients with PSA equal to or below 20 ng/ml, as less than 1% of these patients have detectable bone lesions. Positron-emitting radionuclide scans are also generally not used in prostate cancer staging.
The choice of therapeutic modalities utilized in prostate cancer treatment frequently follow a relatively complicated algorithm as treatment decisions rely on multiple factors including stage, patient’s life expectancy, serum PSA and comorbidities (See National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology for Prostate Cancer, referenced below). In general, for a man with clinically localized prostate carcinoma in whom curative intent is desired, radical prostatectomy and radiation therapy are the primary options. Radical prostatectomy is the mainstay of primary treatment for clinically localized prostate carcinoma. It can also be performed after hormonal therapy and as salvage treatment after failure of radiation therapy. Radiation therapy, with external beam radiotherapy, or implantation of radioactive seeds (brachytherapy), can also be used as a primary modality to treat prostate carcinoma. Expectant management, or active surveillance, in which patients are under close follow-up and definitive therapies, is deferred until there is a sign of disease progression. It is most often selected for older men with a life expectancy of less than 10 years who have low-grade or intermediate-grade (Gleason score < 7) and low-volume prostate carcinoma that is confirmed after extensive prostate sampling. For disseminated disease, therapies are non-curative and include hormone ablation (surgical via orchiectomy or medical anti-androgens).
Traditionally, prostate cancer risk assessment after prostatectomy, has most commonly used a scheme (D’Amico et al) that stratifies patients into low-risk (stages T1c to 2a, and serum PSA less than 10 ng/mL, and Gleason score of 6 or less), intermediate-risk (stage T2b, or serum PSA between 10 and 20 ng/ mL, or Gleason score of 7), and high-risk (stage T2c, or serum PSA greater than 20 ng/mL, or Gleason score of 8 or greater) groups. The fraction of men free of prostate cancer 10 years after radical prostatectomy for these risk categories: 83% of men with low-risk prostate cancer, 46% of men with intermediate-risk prostate cancer, and 29% of men with high-risk prostate cancer. More recently additional risk groupings based on Gleason pattern has been proposed as follows:
- Grade group 1 (Gleason Score 3+3=6)
- Grade group 2 (Gleason Score 3+4=7)
- Grade group 3 (Gleason Score 4+3=7)
- Grade group 4 (Gleason Score 4+4=8)
- Grade group 4 (Gleason Score 3+5=8)
- Grade group 4 (Gleason Score 5+3=8)
- Grade group 5 (Gleason Score 4+5=9)
- Grade group 5 (Gleason Score 5+4=9)
- Grade group 5 (Gleason Score 5+5=10)
Supplementary Questions
- Which of the following statements is true?
- Carcinomas that typically lack both CK7 and CK20 immunohistochemical labeling include hepatocellular, pancreas, prostate, and renal cell.
- Distinct histologic variants of prostate adenocarcinoma include atrophic, pseudohyperplastic, microcystic, foamy gland, mucoid, and signet ring cell.
- Metastatic prostatic adenocarcinoma most commonly involves the liver.
- Sensitivities for PSA and NKX3-1 are higher in some prostate carcinoma variants such as small cell carcinomas of the prostate.
- The absence of diffuse immunohistochemical labeling for PSA in a metastatic adenocarcinoma excludes the possibility of a prostate primary.
- A 52-year-old otherwise healthy man is found to have prostatic adenocarcinoma, Gleason score 8 (4+4), on
prostate needle biopsy performed due to an abnormal digital rectal exam and PSA level of 3.5 ng/ml. Which of the
following statements is most accurate?
- He should have a bone scan, as his PSA level would indicate a high risk of bone metastases.
- Hormone ablation (surgical via orchiectomy or medical anti-androgens) is the most common initial treatment in relatively young patients with localized disease.
- Radiation therapy, with external beam radiotherapy or implantation of radioactive seeds (brachytherapy), would not be appropriate here as it is only used as “salvage” treatment after failure of a primary treatment modality.
- Radical prostatectomy is the mainstay of primary treatment for clinically localized prostate carcinoma.
- This patient is a good candidate for expectant management due to his life expectancy of greater than 10 years and high Gleason score.
- Which of the following histomorphologic features is not common in prostatic adenocarcinoma?
- Abundant mitotic figures
- Blue tinged mucin
- Cribriform structures
- Luminal crystalloids
- Straight luminal borders
References
- Bhargava R. Chapter 8 - Immunohistochemistry of metastatic carcinoma of unknown primary site. In: Dabbs D, ed. Diagnostic immunohistochemistry. 4th ed. Philadelphia, PA: Elsevier; 2014.
- Conner JR, Hornick JL. Metastatic carcinoma of unknown primary: Diagnostic approach using immunohistochemistry. Adv Anat Pathol. 2015;22(3):149-167
- D'Amico AV, Whittington R, Malkowicz SB, et al. Predicting prostate specific antigen outcome preoperatively in the prostate specific antigen era. J Urol. 2001;166(6):2185-2188.
- Kryvenko ON, Epstein JI. Changes in prostate cancer grading: Including a new patient-centric grading system.
Prostate. 2016;76(5):427-433.
- Moch H, Humphrey PA, Ulbright TM, Rueter VE. WHO Classification of Tumours of the Urinary System and Male Genital Organs. 4th edition, Lyons France, IARC Press, 2016.
- Mohler JL. NCCN clinical practice guidelines in oncology (NCCN guidelines®) prostate cancer. http://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf . Published National Comprehensive Cancer Network®. Updated Version 1.2016.
- Nelson WG. Chapter 84 - Prostate cancer. In: Niederhuber JE, ed. Abeloff's Clinical Oncology. 5th ed. Philadelphia PA; Elsevier: 2014.
- Netto GJ. Chapter 16 - Immunohistology of the prostate. In: Dabbs D, ed. Diagnostic immunohistochemistry. 4th ed. Philadelphia PA: Elsevier; 2014.
- Srigley JR, Humphrey PA, Amin MB, Chang SS, Epstein JI. CAP protocol for the examination of specimens from patients with carcinoma of the prostate gland. http://www.cap.org/apps/docs/committees/cancer/cancer_protocols/2012/Prostate_12protocol_3200.pdf. Updated June 2012. © 2012 College of American Pathologists (CAP). All rights reserved.
- Zhou M. Chapter 2 - Neoplastic diseases of the prostate. In: Zhou M, ed. Genitourinary Pathology. 2nd ed. Philadelphia, PA: Elsevier; 2015.
Author
2016
H. Parry Dilworth, MD
CAP Surgical Pathology Committee
Hospital Pathology Associates
Minneapolis, MN
Answer Key
- Distinct histologic variants of prostate adenocarcinoma include atrophic, pseudohyperplastic, microcystic, foamy gland, mucoid, and signet ring cell. (b)
- Radical prostatectomy is the mainstay of primary treatment for clinically localized prostate carcinoma. (d)
- Abundant mitotic figures (a)