Clinical Summary
A 24-year-old woman presents for a routine prenatal visit at five months’ gestation. During her exam a palpable 1.0 cm mass is noted in her right breast. A follow-up ultrasound shows a circumscribed, 1.6 cm hypoechoic nodule. An ultrasound-guided core biopsy is performed. Three months after an uneventful delivery, a 2.2 cm circumscribed, unencapsulated nodule with a markedly myxoid, light yellow-tan cut surface is excised.
Master List
- Fibromatosis
- Myofibroblastoma
- Myxofibrosarcoma
- Nodular fasciitis
- Spindle cell metaplastic carcinoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2013, case 38, and is nodular fasciitis.
Criteria for Diagnosis and Comments
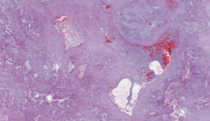
Sections reveal a poorly demarcated tumor composed of short, randomly oriented fascicles of bland, plump spindle cells, which lack pleomorphism and hyperchromasia. The stroma has a loose, tissue culture-like, somewhat myxoid appearance without a significant amount of collagen. Many mitotic figures are present but there are no atypical mitoses. Chronic inflammatory cells as well as extravasated red blood cells can be seen throughout the tumor. Immunostains reveal the tumor to be negative for cytokeratin, S-100 and desmin. The tumor is moderately positive for actin. These histologic features are those of nodular fasciitis.
Nodular fasciitis is a benign mass-forming proliferation of fibroblasts and myofibroblasts. The gross appearance of this lesion is that of a solitary mass which may be circumscribed or infiltrative but not encapsulated. The cut surface may appear myxoid, particularly in early nodular fasciitis, or it may be more fibrous in long-standing lesions. Occasionally central, cystic changes may be seen. The immunohistochemical staining pattern is typical of a fibroblastic or myofibroblastic process. Nodular fasciitis stains positively for smooth muscle actin, muscle specific actin and calponin. These lesions are usually negative for desmin, cytokeratin and S-100.
Clinically this lesion presents as a rapidly growing, frequently painful or tender mass that usually reaches 2.0-3.0 cm in size but rarely exceeds 5.0 cm. Nodular fasciitis most commonly occurs in young adults but can be seen in patients ages 20-50. There is no gender predilection. This lesion is generally located in superficial subcutaneous tissues of the upper extremities, trunk, head and neck with the most common location being the forearm. However, nodular fasciitis can occur anywhere including the breast where it typically arises in the subcutis, and rarely within the breast parenchyma. When nodular fasciitis does occur in the breast, it often mimics breast malignancy radiologically, clinically and on gross examination. Although these lesions are benign and will spontaneously regress, the clinical scenario typically leads to biopsy and local excision. Treatment for this lesion is conservative and includes observation or simple excision. Nodular fasciitis does not metastasize and local recurrence occurs less than 2% of the time.
The etiology of nodular fasciitis is unknown. It was initially thought that this was a reactive lesion caused by trauma, but a history of trauma is only reported in 10-20% of cases. There is some evidence that nodular fasciitis is clonal and thus neoplastic since chromosomal abnormalities have been detected by cytogenetic analysis in some cases; however, this evidence is limited.
Other spindle cell lesions of the breast should be considered in the differential diagnosis, and include both malignant and benign entities. Spindle cell metaplastic carcinomas may mimic nodular fasciitis, but typically demonstrate more nuclear atypia. There is a fibromatosis-like variant of spindle cell metaplastic carcinoma that is also in the differential diagnosis. This entity is composed of plump and elongated spindle cells which infiltrate the stroma. These lesions exhibit minimal nuclear atypia and a low mitotic rate. The fibromatosis-like variants are often associated with an adjacent papillary lesion or radial scar. Lymphoplasmactyic infiltrates may be seen around the edges of this lesion, similar to fibromatosis. Metaplastic carcinomas (including the fibromatosis-like variant) are cytokeratin positive in stark contrast to nodular fasciitis and other benign spindled breast masses, illustrating the importance of immunohistochemistry in the evaluation of these lesions.
Myxofibrosarcoma may rarely occur in the breast; however, it more commonly presents as a painless, slowly growing mass in the extremities of elderly people. It displays a spectrum of cellularity, nuclear pleomorphism and mitotic activity, and the lower-grade variety can be mistaken for nodular fasciitis. Most myxofibrosarcomas are found in the subcutaneous tissues, tend to be multinodular and display low cellularity. This lesion is composed of atypical spindle to stellate cells with ropey vasculature in a myxoid background without appreciable collagen, similar to early nodular fasciitis. These cells generally are more hyperchromatic than the cells composing nodular fasciitis and there is less mitotic activity than is seen in nodular fasciitis. Extravasated red blood cells are not a feature of myxofibrosarcoma. Immunohistochemistry shows positive reactivity for vimentin. Muscle specific actin and smooth muscle actin may be focally positive suggesting myofibroblastic differentiation similar to nodular fasciitis.
Fibromatosis of the breast typically presents as a palpable, radiographically suspicious, stellate infiltrative mass in young women, average age of 45 years. Some patients with fibromatosis have a history of previous trauma to the area, including prior breast augmentation with implants. Histologically this lesion is composed of a spindle cell proliferation with variable amounts of collagen deposition and elongated vessels. The cells show minimal nuclear atypia and lack significant mitotic activity. Scattered lymphoid aggregates are frequently present, located predominately around the periphery. Immunohistochemistry shows positive reactivity for actin, desmin and nuclear staining for beta-catenin, while cytokeratin and CD34 are negative. Wide local excision is the recommended treatment, since the local recurrence rate can range up to 27%.
Another benign spindle cell proliferation of the breast included in the differential diagnosis of nodular fasciitis is myofibroblastoma. This lesion presents as a solitary nodular breast mass averaging 2.0 cm in size, typically subareolar in location and more frequently occurring in men. The lesion is characterized as a proliferation of spindled cells with uniform, bipolar nuclei separated by hyalinized collagen bundles. Only rare mitotic activity is seen in these lesions. Myofibroblastomas also show staining for desmin and actin with absent cytokeratin reactivity, but are beta-catenin negative, and CD34 positive (in contrast to fibromatosis). Local excision is the recommended treatment.
Supplementary Questions
- Which term least accurately describes the possible gross appearance of nodular fasciitis?
- Circumscribed
- Encapsulated
- Fibrous
- Infiltrating
- Myxoid
- Which of the following statements is correct regarding fibromatosis of the breast?
- Fibromatosis may rarely occur following breast trauma
- Fibromatosis shows positive staining for CD34
- Fibromatosis typically occurs in a subepithelial location
- These lesions are typically found in association with a papillary lesion or radial scar
- This lesion is associated with a variable mitotic rate
- Which of the following is a false statement?
- Nodular fasciitis may be brought about by trauma
- Nodular fasciitis may have numerous mitoses
- Nodular fasciitis rarely exceeds a maximum size of 5.0 cm
- The classic histologic appearance of nodular fasciitis is that of tissue culture-like fibroblasts
- The most common location for nodular fasciitis is the trunk
References
- Brown V, Carty NJ. A case of nodular fascitis of the breast and review of the literature. Breast. 2005;14(5):384-387.
- Folpe AL, Inwards CY, eds. Bone and Soft tissue Pathology: A Volume in the Foundations in Diagnostic Pathology Series, Saunders; 2010.
- Hayashi H, Nishikawa M, Watanabe R, et al. Nodular fasciitis of the breast. Breast Cancer. 2007;14(3):337-339.
- Iwatani T, Kawabata H, Miura D, Inoshita N, Ohta Y. Nodular fasciitis of the breast. Breast Cancer. 2012;19(2):180-182.
- Ozben V, Aydogan F, Karaca FC, et al. Nodular fasciitis of the breast previously misdiagnosed as breast carcinoma. Breast Care (Basel). 2009;4(6):401-402.
- Tse GM, Tan PH, Lui PC, Putti TC. Spindle cell lesions of the breast-the pathologic differential diagnosis. Breast Cancer Res Treat. 2008;109(2):199-207.
- Weiss S, Goldblum J. Enzinger and Weiss's Soft Tissue Tumors. 5th ed. Mosby; 2008:312.
Authors
2013
Leah Dvorak, MD
Pathology Resident
University of Minnesota
Minneapolis, MN
Tamera Lillemoe, MD
Surgical Pathology Committee
Allina Health Laboratories
Hospital Pathology Associates
Minneapolis, MN
Answer Key
- Encapsulated (b).
- Fibromatosis may rarely occur following breast trauma (a).
- The most common location for nodular fasciitis is the trunk (e).